 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
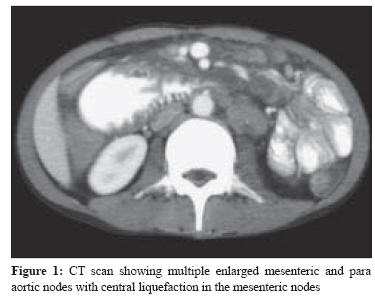
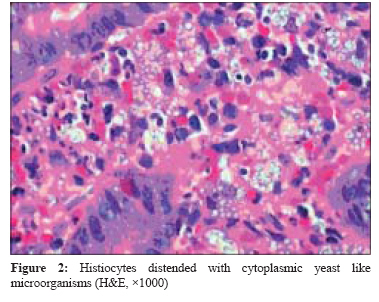
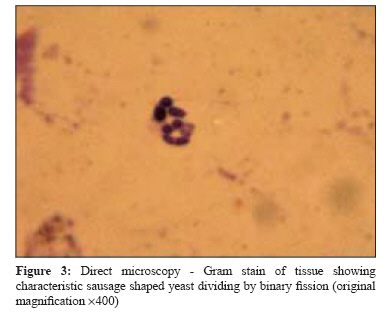
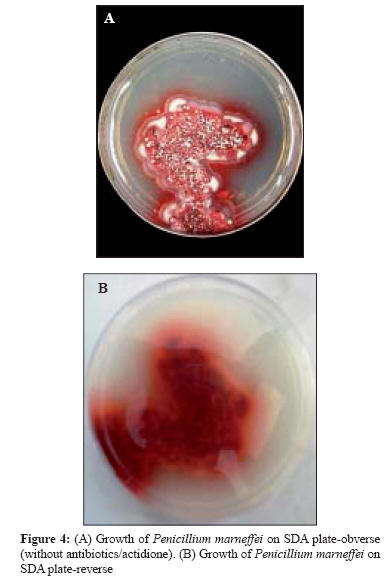
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 180-182 Case Report Acute abdomen: An unusual presentation of disseminated Penicillium marneffei infection George IA, Sudarsanam TD, Pulimood AB, Mathews MS Department of Medicine, Christian Medical College and Hospital, Vellore - 632 004, Tamil Nadu Date of Submission: 09-Oct-2007 Code Number: mb08051 Abstract Varied clinical presentations of Penicillium marneffei , an opportunistic pathogen in HIV disease has been rarely described in literature. We report a patient with advanced AIDS who presented to us with prolonged fever and had features of an acute abdomen. On radiologic imaging he had features of intestinal obstruction and mesenteric lymphadenitis. A diagnosis was made possible by endoscopic biopsies of the small bowel and bone marrow culture which grew P . Marneffei . He was treated with intravenous amphotericin for 2 weeks followed by oral itraconazole. This case is reported for its rarity and unusual presentation and to sensitise clinicians and microbiologists to consider this as an aetiology in patients with advanced HIV/AIDS who present with acute abdomen, more so in patients from a distinct geographic region - South-East AsiaKeywords: Acute abdomen, HIV/AIDS, intestinal mycosis, Penicillium marneffei Infection with Penicillium marneffei , an emerging facultative intracellular dimorphic fungus is an important disease among HIV infected persons in South East Asia. [1] In South East Asian countries like Thailand after extrapulmonary tuberculosis and Cryptococcus , Penicilliosis Marneffei (PM) ranks as the third most common opportunistic infection in people with AIDS. [2] Although Penicillium marneffei has been reported in varied clinical manifestations in India, [3] it has rarely been implicated as a cause of intestinal mycosis. [4] We report a patient with AIDS who presented with features of an acute abdomen wherein a diagnosis of disseminated Penicillium marneffei was made possible by endoscopic biopsies. Case Report A 33-year-old man from Meghalaya, in North East India, presented to the emergency department with insidious onset but rapidly progressing symptoms of severe abdominal pain and vomiting for duration of four days. He also had a few episodes of haemetemesis and malaena over the previous two days. On further asking he complained of fever, loss of appetite, loss of weight of 10 kg and vomiting for three months. He was advised a course of empiric antituberculous therapy two months ago by physicians near his home town, while being evaluated for fever and weight loss, which he discontinued after a month.On physical examination, he appeared pale and chronically ill. Temperature was 100°F, pulse rate was 96/minute and blood pressure was 120/80 mm of Hg. Apart from oral candidiasis and a single 1 x 2 cm axillary lymph node, general examination was non-contributory. His abdomen examination revealed evidence of generalized guarding and tenderness with accelerated bowel sounds. Other systemic examination was normal. On admission his haemoglobin was 10.5 g/dL, total count was 5400 cells/mm 3 (neutrophils 95%) and platelets were 54000 cells/mm 3 . His biochemical parameters were normal. His liver function tests were normal except for a low albumin of 2.2 g%. Serum ELISA for HIV-1(Human immunodeficiency virus-1) was positive and subsequently his CD4 counts came as 7 cells/mm 3 . Plain radiographs of the abdomen were non-contributory and a Computed Tomogram (CT) of the abdomen showed marked mucosal thickening and narrowing of the third part of duodenum with proximal dilatation suggestive of partial obstruction at that site. There were multiple enlarged mesenteric and paraaortic nodes with central liquefaction in the mesenteric nodes and mild ascites [Figure - 1]. An urgent surgical consultation was obtained and conservative management was advised. Subsequently, he underwent a gastroscopy which showed oesophageal candidiasis and nodular erythematous friable folds in the second part of the duodenum with narrowing of the lumen. The endoscopic biopsies from the duodenum showed broadening and mild blunting of villi with oedema of the lamina propria and aggregates of histiocytes, admixed with plasma cells, lymphocytes and neutrophils. The cytoplasm of the histiocytes was packed with yeast like microorganisms [Figure - 2] that stained positive with the Periodic Acid Schiff (PAS) and Gomori Methanamine Silver (GMS) stains. In the microbiology laboratory, direct microscopy of the tissue sample revealed typical septate sausage shaped cells pathognomonic of P. marneffei [Figure - 3]. Culture of the duodenal tissue grew Penicillium marneffei . The bone marrow also grew Penicillium marneffei [Figure - 4]A and B, on the 6 th day of incubation at a temperature of 28 degree celsius. The patient was treated with amphotericin B at a dosage of 0.6 mg/kg/day intravenously for two weeks, followed by a 400-mg/day dosage of oral itraconazole for 10 weeks, as per the current recommendations. [5] It was decided to initiate anti retroviral therapy from a hospital near his home town after 2 weeks. Discussion Penicillium marneffei is a dimorphic fungus that causes life-threatening disseminated infection, Penicilliosis Marneffei (PM), in a geographically distinct area of the world - South-East Asia. The disease has been reported among HIV-infected persons in Thailand, Myanmar (Burma), Vietnam, Cambodia, Malaysia, north-eastern India, Hong Kong, Taiwan and southern China. [1] The infection is acquired by inhalation of conidia from an environmental source like soil. In a study from Thailand of 92 culture proven cases of PM, CD4+ cell count at the time of the diagnosis was consistently less than 50 cells/mL. The most common presenting symptoms and signs were fever (in 99% of the patients), anaemia (78%), pronounced weight loss (76%), generalized lymphadenopathy (58%) and hepatomegaly (51%). [2] Generalised lymphadenopathy, splenomegaly and osteoarticular lesions and pericarditis have been described. [6] Our patient, in addition to the usual presentations of chronic fever and weight loss, presented with an acute abdomen with partial intestinal obstruction and mesenteric lymphadenitis.To our knowledge, this is the first case of an acute abdomen in an HIV infected adult due to Penicillium infection. Ukarapol reported two cases of HIV-infected children with mesenteric lymphadenitis who presented with prolonged fever and abdominal pain that were initially diagnosed as peritonitis and acute appendicitis prior to exploratory laparotomy. [7] Ko and colleagues [4] have described three cases of intestinal penicilliosis diagnosed by endoscopic biopsy. However none of these patients had a clinical presentation with an acute abdomen as this patient did. Information on the outcome and response to treatment unfortunately was not possible in this case as the patient was from far and was lost to follow-up. This would have given further credence to the case. In patients with advanced HIV/AIDS who present with acute abdomen, opportunistic fungal infections of the bowel especially penicilliosis needs to be considered as aetiology, more so in patients from a distinct geographic region - South-East Asia. Acknowledgement We wish to acknowledge the help of colleagues in all three departments who helped in the diagnosis and management of this patient. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08051f4.jpg] [mb08051f1.jpg] [mb08051f2.jpg] [mb08051f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}