 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
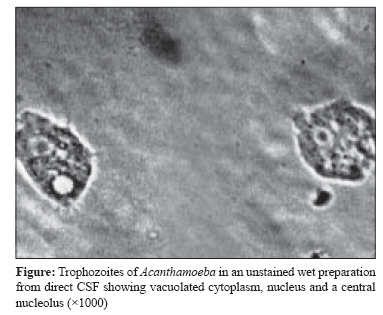
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 182-184 Case Report Acanthamoeba encephalitis Kaushal V, Chhina DK, Kumar R, Pannu HS, Dhooria HPS, Chhina RS Department of Microbiology, Dayanand Medical College and Hospital, Ludhiana - 141 001, Punjab Date of Submission: 02-Aug-2007 Code Number: mb08052 Abstract Central nervous system infection with free-living amoebae is rare. We present a fatal case of Acanthamoeba encephalitis in a 63-year-old female from India where acanthamoebae were demonstrated and cultured from CSF. In spite of treatment with amphotericin B, fluconazole and rifampicin the patient did not survive. Amoebic infection should be suspected in a patient of encephalitis of unexplained aetiology as timely diagnosis can lead to a favourable outcome. Keywords: Acanthamoeba, encephalitis Amoebic encephalitis is an infrequently encountered, mostly fatal, infection of the central nervous system (CNS) seen in both normal and immunocompromised individuals. Granulomatous amoebic encephalitis (GAE) caused by Acanthamoeba spp. and Balamuthia mandrillaris and primary amebic meningoencephalitis (PAM) caused by Naegleria fowleri are the two clinical manifestations of CNS amoebic infection. More than 400 cases have been reported in world literature with only two to three percent survival. Acanthamoebae spread haematogenously from upper respiratory tract or skin lesions into brain parenchyma. [1] The course of amoebic encephalitis is typically subacute, with altered mental status, headache, fever, neck stiffness, seizures, focal neurological signs such as cranial nerve palsies and coma leading to death within one week to several months after onset. Limited awareness among the clinicians and laboratory personnel delay the diagnosis of GAE and lack of timely and effective antimicrobial therapy usually lead to a fatal outcome. All these factors, combined with low autopsy rate in such deaths, are largely responsible for rare incidence of this disease. There are reports from India where acanthamoebae were either demonstrated in direct CSF or on autopsy but there are very few reports where these have been successfully cultured from CSF. [2],[3] The present case report highlights the importance of including amoebic encephalitis in differential diagnosis of pyogenic meningitis/encephalitis when cerebrospinal fluid (CSF) examination is negative for routine organisms and treatment with conventional anti meningitis drugs has failed. Case Report A 63-year-old woman was hospitalised with a history of vomiting for five days, headache, decreased appetite and altered sensorium for 15 days. She was hypertensive for the last 20 years and was on irregular treatment. On admission she was restless, drowsy and afebrile. She was moving all limbs but neck rigidity was present. Her pulse rate was 94 per minute and blood pressure was 140/90 mmHg. She had no skin lesions or any other traumatic break in the skin. Chest X-ray showed left lower zone pneumonitis. Oral candidiasis was present. Serum alkaline phosphatase was 123 IU/L and ammonia was 107 mg/dL. CSF examination revealed: proteins 26 mg/dL, glucose 96 mg/dL and leukocytes 10/mm 3 most of which were lymphocytes. On Gram staining, CSF smears showed no bacteria and no yeast cells. India ink preparation was negative. Bacterial and cryptococcal antigen latex agglutination tests were negative. CSF cultures were negative for bacteria and fungi. Plain CT scan of head was normal. A tentative diagnosis of left lower lobe pneumonitis with sepsis and hepatic encephalopathy was made and treatment with ampicillin 1G intravenously six hourly and cefoperazone-sulbactum 2G intravenously twice a day was started. However she did not show improvement and her meningeal signs persisted. 10 days post admission a repeat CSF sample showed presence of a few abnormally large cells on Gram stain. No bacteria or yeast were seen. The wet preparation of the CSF revealed few organisms with amoeboid movement morphologically suggestive of trophozoites of Acanthamoeba species. These cells had an irregular shape, vacuolated cytoplasm and a single nucleus located centrally or slightly eccentrically [Figure - 1]. Giemsa stained smear confirmed the presence of amoebae with few of them undergoing binary fission. CSF sample was cultured on non-nutrient agar medium seeded with an unspecified strain of Escherichia coli . After 48 hours, the culture plates showed a prolific growth of Acanthamoeba trophozoites. A wet preparation from this plate revealed many motile trophozoites with characteristic acanthopodia. On prolonged incubation the plates showed presence of numerous cystic forms. CSF culture for pyogenic organism and the fungus was negative.After confirming the presence of Acanthamoeba in CSF sample by culture, treatment was started with amphotericin B 10 mg, intravenously and the dose was subsequently increased to 30 mg, along with rifampicin 450 mg once a day and co-trimoxazole but the latter two drugs had to be withdrawn after a week as the patient developed acute gastritis. She showed improvement over the week and started accepting oral feeds but her sensorium again worsened. Her CSF sample examined two weeks later revealed the persistence of Acanthamoeba . Inj fluconazole 100 mg intravenously twice a day was added but patients′ attendants requested leave against medical advice and she finally expired in a private nursing home after four months of her initial presentation. Discussion Free-living amoebae are ubiquitously present and are capable of causing human disease. Naegleria fowleri , Acanthamoeba species and Balamuthia mandrillaris are known to cause CNS infection in immunocompromised and rarely in immunocompetent hosts. [4],[5] Acanthamoeba spp. are the causative agents of amoebic keratitis - a painful sight threatening disease of eyes and granulomatous amebic encephalitis, a fatal disease of the central nervous system. Acanthamoeba meningoencephalitis is a slowly progressive infection with an insidious onset. The course is typically subacute with altered mental status, headache, fever, neck stiffness, seizures, focal neurological signs such as cranial nerve palsies and coma leading to death within 1 week to several months after onset. Occasional survivors of this disease have also been reported. [4],[5] The portal of entry of amoebae may be break in skin or respiratory tract or by inhalation of wind blown cysts with subsequent spread to CNS through the circulatory system. [1] This patient might have acquired the infection through the respiratory route. Human infections have increased significantly in last 15 years. The infection occurs mostly in patients undergoing immunosuppressive therapy or other immunocopromised patients such as AIDS patients or patients with systemic lupus erythematosus, chronic alcoholics, debilitated and malnourished individuals but according to one of the recent reports from Germany Acanthamoeba infection was seen in an immunocompetent woman. [5] No immunocompromising condition was present in our patient also.Amoebic encephalitis is almost always fatal because of difficulty and delay in diagnosing the disease and lack of optimal antimicrobial therapy. The documented cases of this infection may be low because of difficulty in diagnosis and lack of clinical suspicion of this subacute disease that mimics bacterial leptomeningitis, tuberculous meningitis or viral encephalitis. As a result, the disease remains largely undetected in both industrialized and non-industrialized nations making it a cause of concern for clinical and laboratory personnel and parasitologists. There have been reports of misidentification of organisms as reactive histocytes [6] or yeasts [7] or failure to recognize amoebae leading to misdiagnosis. [8] A similar situation might have been present in the present case had the second CSF sample not been sent to the laboratory and those abnormal cells were not noticed in the wet preparation. In another case report, amoebic trophozoites were detected in a routine cytological examination of CSF sample leading to early diagnosis of GAE and subsequent survival of the patient. [5] So it is necessary to have a high index of suspicion to recognize this infection, especially when CSF examination is negative for routine organisms and treatment with conventional antibiotics fails. [3] Some investigators have used serological and molecular diagnostic methods [9] that are non-invasive but are time-consuming, expensive and need further evaluation. CT and MRI imaging findings have also been found useful in diagnosis of GAE [10] but no significant finding in CT scan head was observed in this patient. There is no known effective therapy for this disease. Various treatment regimens have been tried for GAE but therapeutic success has been elusive in most of the cases. The drugs that have been tried in varied combinations include amphotericin-B, rifampicin, trimethroprim-sulfamethoxazole, ketokonazole, fluconazole, sulfadiazine, albendazole etc. Timely diagnosis, early initiation of antimicrobial therapy, virulence of the agent and host immune factors all play a role in determining the outcome of GAE. The current report highlights the importance of including GAE in differential diagnosis of any patient with subacute central nervous system syndrome with no known cause. It is more common especially in patients with compromised immunity. Increasing familiarity of the clinicians, clinical microbiologists and pathologists with infections due to free living amoebae will certainly help in more aggressive diagnosis and reporting, understanding of the risk factors, improvement in therapeutic interventions and prevention of fatal outcomes in such cases. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08052f1.jpg] |
| |||||||||
{kind=link}