 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
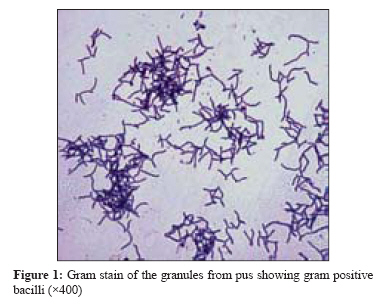
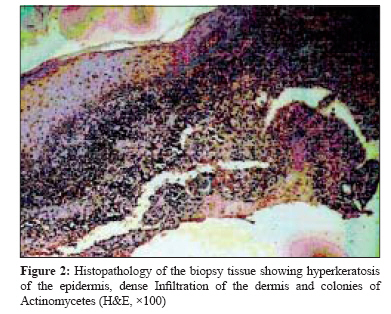
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 184-186 Case Report Primary cutaneous actinomycosis: A rare soft tissue infection Metgud SC Department of Microbiology, Jawaharlal Nehru Medical College, Belgaum - 590 010, Karnataka Date of Submission: 10-Jul-2007 Code Number: mb08053 Abstract Actinomycosis caused by Actinomyces spp. is a chronic and suppurative infection caused by an endogenous gram positive bacterium. The unusual sites of infection are the head and neck, thorax and abdomen and are almost always endogenous in origin. Primary cutaneous actinomycosis is very rare and is usually associated with external trauma and local ischemia. We report a case of a primary cutaneous actinomycosis of the thigh in a 30-year-old man. The patient acquired the infection through an injection wound which progressed to multiple discharging sinuses. Clinical material from the wound demonstrated the presence of Actinomyces in smears and cultures. The patient was diagnosed and successfully treated with surgical resection and combined antibiotic therapy.Keywords: Injection wound, primary cutaneous actinomycosis Actinomycosis is an anaerobic, gram positive bacterial infection, seen in different parts of the body. Actinomycosis is caused in humans by Actinomyces israelii and in animals by A. bovis , A. naeslundii and A. viscosus have been documented. The infection is commonly seen in tropical countries and characterised by chronic and progressive suppurative inflammation, typically presenting as cervicofacial, thorax and abdomen lesions. Primary cutaneous actinomycosis is a rare entity and the diagnosis requires a high index of suspicion. Primary disease of extremities is uncommon and mostly has an association with trauma and bites. Case Report A 30-year-old healthy man with swelling in back of the left thigh since 10 months was referred by the local surgeon to a private hospital in Belgaum for further treatment as his swelling started increasing with granular pus for which he had consulted the doctor. Prior to this, the patient had visited a village doctor, who had prescribed an oil-based ointment for local application and advised him hot fomentation with some plant leaves soaked in oil. He gave history of taking an injection followed by which he developed the swelling measuring around 1 cm in size, which started increasing in size and occupied almost whole of the back of the thigh- approximately 15 cm in size and later on he developed multiple discharging sinuses. The lesion was dusky red, firm fluctuating nodules with white to yellowish thick granular pus. The pus sample was sent to our department for culture and sensitivity.The sample was scanty, thick in consistency and yellowish in colour though no offensive smell was noticed. Gram stain of the sample was performed, which showed plenty of pus cells with non-sporing, long, gram positive bacilli. As the sample was not sufficient we requested for a fresh sample. Few yellowish granules were obtained which were washed in saline and centrifuged. Small drop of the deposit was collected on a clean grease free slide and crushed between the slides and direct wet mount as well as Gram stain of the same was performed which revealed gram positive bacilli with polymorphonuclear cells [Figure - 1]. The fresh sample was inoculated on two sets of blood, chocolate and MacConkey′s agar. One set was incubated aerobically and the other set in a candle jar at 37°C. Anaerobic incubation was not done due to lack of facilities. While no growth was seen on plates incubated aerobically minute translucent colonies were observed on blood and chocolate agar plates incubated in a candle jar after 72 hours. The Gram stain of the same showed similar gram positive bacilli as seen in the clinical sample [Figure - 1]. The cold acid fast stain using 1% H 2 SO 4 was negative. The isolate was identified up to genus level as Actinomyces spp. using standard methods. [1] All other test results including blood biochemistry, haematology, urine analysis and stool examination were within normal limits. The histopathology of the biopsy tissue showed ray fungus surrounded by polymorphonuclear leucocytes associated with hyperkeratosis of epidermis and dermal infiltration, which corroborated the microbiological findings [Figure - 2]. Antibiotic sensitivity by disc diffusion method showed resistance to ampicillin and sensitivity to cefuroxime and co-trimoxazole. The wound debridement was done and the patient was treated with intravenous Penicillin G 6 million units qid for 4 weeks and oral cotrimoxazole 960 mg BD 4 weeks along with supportive treatment comprising of daily dressing, multivitamins, iron supplement and NSAIDs. The patient showed a drastic improvement. The lesion started regressing with no discharge. The patient was discharged and advised to come for follow-up after one month. After one month the swelling had subsided completely with no discharge. Discussion Actinomycosis occurs worldwide, with likely higher prevalence rates in areas with low socioeconomic status and poor dental hygiene. For unknown reasons, men are affected more commonly than women, with the exception of pelvic actinomycosis. The reported male-to-female ratio is 3:1. [2] They belong to the order of Actinomycetales, family Actinomycetaceae and genus Actinomyces . Members of the genera Propionibacterium, Actinobacillus and Bifidobacterium may cause similar clinical syndromes. These bacteria grow slowly in anaerobic-to-microaerophilic conditions, forming colonies with a characteristic molar tooth appearance. The most commonly isolated species is Actinomyces israelii . We were able to isolate the organism in a candle jar, which is easily available and provides microaerophilic conditions. Therefore, we believe that this organism can be isolated and identified even in a laboratory with no facilities for anaerobic culture.Almost all actinomycotic lesions contain so-called companion bacteria. The most important of these bacteria is Actinobacillus actinomycetemcomitans , followed by Peptostreptococcus, Prevotella, Fusobacterium, Bacteroides, Staphylococcus and Streptococcus species and Enterobacteriaceae , depending on the location of actinomycotic lesions. Actinomycosis is a subacute-to-chronic bacterial infection caused by filamentous, gram-positive, anaerobic-to-microaerophilic bacteria that are not acid fast. It is characterised by contiguous spread, suppurative and granulomatous inflammation and formation of multiple abscesses and sinus tracts that may discharge sulfur granules. The most common clinical forms of actinomycosis are cervicofacial (i.e., lumpy jaw), thoracic and abdominal. In women, pelvic actinomycosis is possible. Actinomyces spp. are prominent among the normal flora of the oral cavity but less prominent in the lower gastrointestinal tract and female genital tract. As these microorganisms are not virulent, they require a break in the integrity of the mucous membranes and the presence of devitalized tissue to invade deeper body structures and cause human illness. Actinomycosis is believed to be acquired by endogenous implantation in to deep tissues where anaerobic conditions prevail. The disease develops in tissue adjacent to the mucosal surfaces that harbour the microorganisms and human actinomycosis most frequently affects the face and neck, but may also be encountered in thoracic and abdominal sites. Punctured wounds, dental extractions or compound fractures are some routes of infection. In these types of infections, there is usually a history of a surgical procedure, to which the source and mode of spread can be traced as the organism becomes pathogenic in the presence of devitalized tissues with reduced oxygen tension. Cutaneous localisations of actinomyces generally occurs by contiguity of underlying foci by direct inoculation or by spread through the bloodstream during a septicaemic phase of the infection. Primary actinomycosis of the extremity is rare because of the exclusively endogenous habitat of the etiologic organism. [3],[4],[5] The majority of the cases reported have had a clear history of trauma, either a human bite or a perforating injury with contamination from outside. [3] In this case the patient had acquired the infection through the injection, but the source is not known. This is more akin to the mode of infection in cases of actinomycetoma, where most of the times a history of puncture wounds can be traced. Cutaneous actinomycosis manifesting with nodular lesion tends to form fistulae and needs to be differentiated clinically from other chronic inflammatory skin diseases, such as cutaneous tuberculosis, sporotrichosis and nocardiosis. The histopathological examination of the lesions is important to confirm the pathology by demonstrating the presence of the organisms and attendant inflammatory changes. Similar cases have been reported from Iran [6] as well as from India. [7] This case report highlights the importance of using sterile disposable syringes at all times. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08053f2.jpg] [mb08053f1.jpg] |
| |||||||||
{kind=link}
{kind=link}