 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
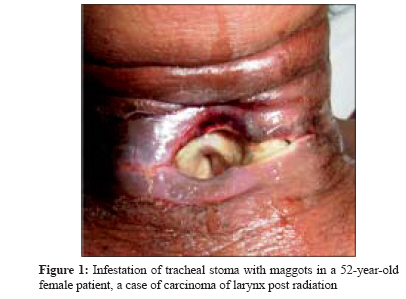
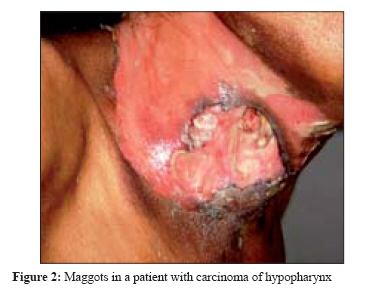
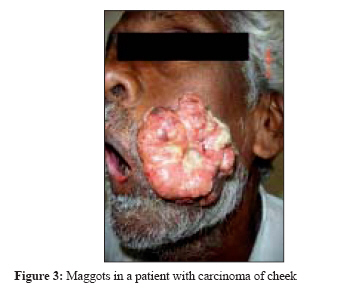
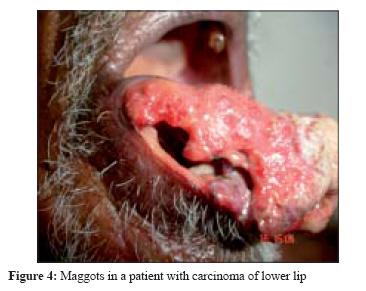
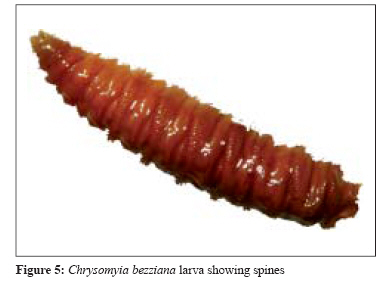
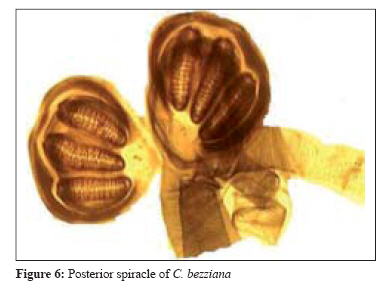
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 189-192 Case Report Myiasis in different types of carcinoma cases in southern India Gopalakrishnan S, Srinivasan R, Saxena SK, Shanmugapriya J Vector Control Research Centre, Indian Council of Medical Research, Pondicherry - 605 006 Date of Submission: 03-Jul-2007 Code Number: mb08055 Abstract Myiasis maggots were isolated from the cancerous wounds, when the patients reported to the Department of ENT-OPD, JIPMER, Pondicherry. Maggots were identified to Chrysomyia bezziana based on characteristic patterns of posterior and anterior spiracles. Although the categories of cancer wounds were different, invasions were due to C. bezziana , which is very common in suburban areas of Tamil Nadu and Pondicherry in southern parts of India. This observation showed the importance of hygiene and sanitation in tropical countries with high fly population and emphasised the need for correct diagnosis of this obligatory myiasis, which was destructive. Through proper health care, further destabilization due to myiasis was avoided.Keywords: Carcinoma cases, Chrysomyia bezziana, myiasis Myiasis, the infestation of live human and vertebrate animals with dipterous fly maggots is common throughout the tropical region. [1] This misery is generally associated with traumatic injury, erosive or ulcerative lesions or haemorrhage. [2] Occurrence and site of invasion of myiasis vary with the sanitary conditions and other environmental factors. Infestation with maggots causes severe pain and mental agony among humans, while hammering economic loss significantly among domestic mammals. [2] Despite the fact that the scourge is very common in rural areas of the tropical region, myiasis has been reported around the world. [3],[4],[5] Severity of myiasis depends on the location of the infestation, lesions and tissue inflammation. Many species of dipterous flies among the genera Chrysomyia and Cochliomyia have been reported to be the most important obligatory myiasis producers among human and/or domestic animals. [6],[7] Infestation with maggots from myiasis of periuretheral area caused by C. bezziana from carcinoma cervix, grade III was reported from central part of India. [6] However, information on species involved in myiasis in southern part of India is scanty. To know the species of dipterous flies involved, an attempt was made to screen and isolate maggots from patients having cancerous wounds. In the present communication four cases of myiasis involving carcinoma of larynx, hyphopharynx, cheek and lower lip are reported for the first time from southern part of India. Case Reports Case 1 Case 2 Case 3 Case 4 Four maggots isolated from each of the patients were preserved in formalin (10%) separately. For identification, two maggots from each batch were washed with distilled water, soaked in 10% sodium hydroxide for 12 hours following which the last segment was cut and the spiracular plate was dissected and mounted in Hoyer′s medium and kept over a hot plate for clearing for two days. Identification was done using the standard key. [2] The maggots were bright pinkish brown in colour and measured 16-18 mm in length and 2-3 mm in width. The body was covered with tough but not sclerotic integument, having bands of dark, robust and thorn like spines. On microscopic examination, the bodies of the maggots isolated from each of the patients were alike and each maggot consisted of eleven apparent segments. All the segments had belts of well developed minute black spines except the anal segment [Figure - 5]. Anterior spiracle showed five finger-like processes. The paired posterior spiracle situated in the cleft on the posterior face of the anal segment had three straight slit-like openings with lateral swellings and a dark peritreme surrounding them [Figure - 6]. The peritreme was incomplete enclosing the poorly defined button, while the anterior spiracles had five finger-like processes. The maggots collected from all the patients were identified to the genus Chrysomyia based on characteristics of the mature larva and patterns of the posterior spiracle. The five finger-like processes of the anterior spiracle helped to confirm the species to bezziana . [6] Chrysomyia bezziana Robineau-Desvody (Diptera: Calliphoridae) recorded from these four patients is an old world screw worm fly maggot. Adults of this fly are free living, while their maggots are parasitic. [8] Discussion Although female flies are attracted to odoriferous suppurating lesions and open wounds, the eggs are deposited on the unbroken, soft skin of various parts of the body that are contaminated by blood or mucous discharge. In addition, the eggs can be transferred into these sites by patient′s own fingers due to poor hygienic habits. Upon hatching, the maggots penetrate deep into tissue aided by their sharp mouth hooks and anchoring inter-segmental spines. The hooked mouthparts and inter-segmental spines scrape away the tissues and lacerate the fine blood vessels, while feeding. During feeding on necrotic or living tissue, the caudal ends of the maggots with their blackish peritremes remain visible at the surface of the lesion, enabling the larvae to breathe. Progressive necroses of muscles continue, associated with larval growth and invasion until a large cavernous lesion is formed, while the larvae aggregate and remain active. Haemorrhage from the lesion is severe and surrounding tissue become tense, oedematous, emitting characteristic pungent odour. Before the occurrence of major functional disturbance associated with extension of the lesion, signs of infestation include presence of ragged, foul smelling lesion containing the maggots. Extension of lesion into body cavity would be seen in some of the cases. Although myiasis causes severe pain in patients who suffer from non-cancerous wound, none of the patients experienced pain/discomfort as the larvae destroyed the sensory nerve endings during the process of invasion in cancer patients. Infestation is common in tropical countries, especially India. [3],[8] Commonly implicated dipterous families include: Muscidae, Sarcophagidae, Calliphoridae, Anisopodidae and Scinoinidae . Larvae of C. bezziana cause obligatory myiasis among human and animal tissues. Genitourinary myiasis in man has been reported to be associated with poor general health and hygiene, restricted mobility, urinary obstruction and ulcerating lesions. [2] However, genitourinary involvement is rare with only one documented case from India. [9] The sites commonly involved in myiasis are nose, ear, tracheotomy wound, face, gums and serous cavities. [4] The pathogenicity results from inflammation and toxin secreted by the larvae which prevents healing. [4] In the patients reported here, it was noticed that the infestations made the patients socially isolated and the patients got into a depressive state. Underlying predisposing factors necessitate correction like improving the nutrition, correction of anaemia and attention to local hygiene. The treatment is simple and involves usage of anti-larval measures (turpentine oil or mixture of turpentine oil and chloroform) followed by removal of the larvae. [10] A broad antibiotic cover is recommended to prevent secondary infections. Our cases illustrate the importance of hygiene and sanitation in tropical countries with high fly population and emphasize the need for correct diagnosis of this obligatory myiasis, which is potentially destructive. Acknowledgements We thank the Director, JIPMER, Pondicherry and Dr. P. Jambulingam, Deputy Director, Vector Control Research Centre, Pondicherry for their support.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08055f6.jpg] [mb08055f5.jpg] [mb08055f3.jpg] [mb08055f2.jpg] [mb08055f1.jpg] [mb08055f4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}