 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
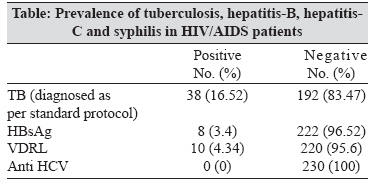
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 196-197 Correspondence Prevalence of tuberculosis, hepatitis B, hepatitis C and syphilis co-infections among HIV/AIDS patients Mahajan A, Tandon VR, Verma S, Singh JB, Sharma M Post Graduate Department of General Medicine, Governmentt Medical College, Jammu - 180 001, Jammu and Kashmir Date of Submission: 13-Jan-2007 Code Number: mb08057 Dear editor, Co-infections of tuberculosis (TB), hepatitis-B (HBV), hepatitis-C (HCV) and syphilis are a major concern in HIV/AIDS patients. TB remains an important public health problem in the world that has been exacerbated by the HIV epidemic, resulting in increased morbidity and mortality wordwide. [1] HIV, HBV and HCV share modes of transmission and hence co-exist in the same host at significantly high rates. [2] Enormous evidences are available indicating that syphilis increases the risk of HIV infection. [3] The prevalence of co-infection with HIV varies widely across different studies within India and outside. Therefore, it is important to find out regional prevalence of these co-infections. Moreover, co-infections with the HIV have become a major health care catastrophe. Hence, it is important to identify them early to reduce the morbidity, delay mortality and improve quality of life in HIV/AIDS patients. According to HIV prevalence rates in adult population, the state of Jammu and Kashmir in India has been placed in low prevalence state. [4] However, in this state the disease has begun to show its ugly face in the recent time [5] and there is a dearth of such data of co-infection in HIV/AIDS patients. This is a prospective study to find out associated infections like TB, HBV, HCV, syphilis in HIV/AIDS patients. HIV/AIDS cases were diagnosed as per the NACO, 2000 criteria. [6] The following screening tests were used to evaluate associated infections, HBsAg micro screen ELISA Test Kit (for hepatitis B); HCV micro ELISA (3 rd generation): for detection of antibodies to Hepatitis C virus in human serum/plasma and Rapid plasma reagin test (RPR Test) for rapid serological diagnosis of syphilis. Tuberculosis was diagnosed as per standard protocol on the basis of sputum smear and culture results for Mycobacterium tuberculosis with clinical and radiographic evidence of tuberculosis (TB). Those with radiographic evidence and sputum negative were given 10 days antibiotic treatment and if disease still persisted they were diagnosed as patients of TB. In selected patients FNAC, MRI, CT scan was carried to confirm the diagnosis. Among 230 HIV/AIDS patients enrolled, 38 (16.52%) patients had TB at some stage of HIV/AIDS infection. HBsAg was positive in eight cases (3.47%); anti Hepatitis C antibody was present in none of the cases. Ten (4.34%) out of 230 cases were positive for VDRL [Table]. CD4 count was less than 200 mm 3 in 73 patients in HIV alone, 20 in TB, six in HBV and five patients in syphilis co-infection group. Sixty patients recorded absolute TLC less than 1200/cm 2 in HIV alone group. Whereas 20, three and four patients recorded absolute TLC less than 1200 mm 3 in TB, HBV and syphilis co infection groups respectively. Among 38 total diagnosed TB co infection patients, clinical evidence was present in 36 (94.73%) whereas, 2 (5.26%) asymptomatic patients were diagnosed by keeping high suspicion using TST. Most common presentation was marked weight loss in 32 (84.21%) followed by fever 30 (78.94%), cough and expectoration in 20 (52.63%). Sputum smear was positive in 14 (36.84%) TB patients co-infected with HIV. Radiographic evidence of TB was seen in 18 patients. Six of these patients had pleural effusion, homogenous opacity with cavity was present in three, mediastinal mass and old healed cavity in two patients each, and hilar lymph node, milliary parttern, multinodular shadow, consolidation and multiple lobulated shadow in hilar region in one patient each. With late HIV infection cases lower lobe involvement was more common whereas, consolidations were more common in early HIV infections. In patients who showed miliary pattern, CD4 count was 16/cm 2 . Pulmonary TB was seen in 17 patients who correlated clinically, radio graphically and with sputum smear positive. Extrapulmonary disease was seen in 19 patients with lymphadenopathy. Cervical and Axillary lymph node involvement was most common. All these were diagnosed by FNAC. Among other sites in CNS, CT-scan diagnosed cyst with edema was seen in one patient and MRI diagnosed space occupying lesion in one, which were confirmed to be tubercular lesion after CSF examination. TB ascitis was diagnosed in two patients, caries spine (D10-D12) with cold abscess in two, C5 vertebral collapse in one and rib TB in one patient. Disseminated form of TB was seen in two patients. In one patient CD4 count was 28/mm 3 , whereas the status was not known in the other. All HBV patients were asymptomatic and syphilis was diagnosed in only 10 patients after performing VDRL in all the HIV diagnosed patients. All diagnosed patients were of primary syphilis. Among the total diagnosed TB co-infection patients, 29 had active disease and were put on ATT. Nine patients had already been treated with ATT after being diagnosed with HIV infection. Patients with HBV were treated with 2NRTIs (Zidovudine + Lamivudine) + 1NNRTI (Efavirenz) and patients with syphilis were treated with Benzathine penicillin G, 2.4 MU IM in a single dose. The patients are on regular follow-up. This study documents fairly high rates of TB, HBV and syphilis co-infection among HIV infected persons. Thus, it should be mandatory to screen every HIV/AIDS patient for co-infection and vice-versa for early detection and a simultaneous treatment besides HIV infection management to combat the menace of this dreadful disease. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08057t1.jpg] |
| |||||||||
{kind=link}