 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
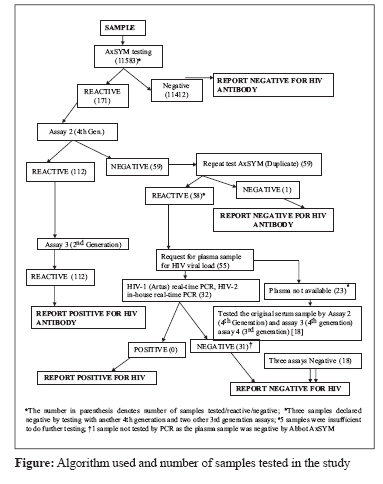
Indian Journal of Medical Microbiology, Vol. 26, No. 2, April-June, 2008, pp. 200-202 Correspondence Experience with a Fourth Generation Human Immunodeficiency Virus Serological Assay at a Tertiary Care Centre in South India Kannangai R, Moorthy M, Kandathil AJ, Sachithanandham J, Thirupavai V, Nithyanandam G, Sridharan G Department of Clinical Virology, Christian Medical College, Vellore 632 004 Tamil Nadu Date of Submission: 25-Sep-2007 Code Number: mb08061 Dear editor, The human immunodeficiency virus (HIV) epidemic continues to be a burden globally especially in developing countries. [1] Though there is dramatic progress in the diagnostic methodologies, the detection of antibodies continues to be the mainstay of diagnosis in most of these countries. The fourth generation HIV serological assays have been in place in developed countries for a few years. However, they have been introduced in the developing countries only recently. In this study, we have looked at the performance of a fourth generation HIV assay in real-time. A total of 11, 583 samples received for HIV screening during 2006 September through December were included in this study. The samples were received from patients who were seen in the out patient facility for any procedures/surgery, antenatal screening or with suspicion of HIV infection. The HIV testing was not anonymous or unlinked because counselling services were offered to those in need. In our hospital, a general consent is obtained for all investigations, including blood tests. The HIV antibody testing was done with the sole purpose of better management of HIV infected individuals; the required medical or surgical treatment was never withheld from any patient. The hospital policy is to refer HIV positive individuals to the infectious disease clinic, where counselling services are offered and further course of action determined. This has been the approach followed at our hospital in accordance with the revised guidelines for HIV counselling, testing and referral by CDC (Centre for Disease Control) as it recommends routine HIV testing of all clients from area where the prevalence is> 1%. [2] All the samples were first screened by the Abbott AxSYM HIV Ag/Ab combo test (Abbot, Wiesbaden, Germany). All negative samples were declared negative. All the HIV reactive samples were tested by another fourth generation assay, Vironostika HIV Uni-Form II Ag/Ab (Biomeriux, Boxtel, Netherlands). If the results of the above two assays were concordant those samples were further tested by a second generation assay, HIV TRIDOT (J Mitra and Co. Pvt. Ltd, New Delhi, India). Samples reactive in all the three assays were reported as positive for HIV antibody. Samples which showed discrepant results in the first two assays were further tested in duplicate by Abbott AxSYM (Abbot, Wiesbaden, Germany) and subsequently by two more serological assays Genscreen HIV Ag/Ab, (BIORAD, Marnes LA Coquette, France), Retrocheck (Qualpro Diagnsotics, Goa, India) or Genscreen HIV-1/2 (BIO RAD, Marnes LA Coquette, France) and molecular assays for HIV-1 and HIV-2. The algorithm followed during the study period is shown in the figure. All the assays used for the detection of HIV antibody/antigen were UNAIDS/WHO approved. The molecular testing carried out included both HIV-1 and HIV-2 RNA detection by a real- time RT-PCR. The HIV-1 RNA was estimated using real-time PCR, Rotor-Gene 3000 (Corbet Research Scientific, Australia) with Artus HIV-1 RG RT-PCR assay (Qiagen GmbH, Germany). The manufacturer′s instructions were followed for extraction of RNA and for further RT-PCR amplification. The assay contains reagents and enzymes for the reverse transcription and specific amplification of a 73-bp region of the LTR region in the HIV-1 genome. The HIV-2 PCR used was an in-house real-time PCR assays with Syber Green chemistry in which a 108-bp product from the envelop region was amplified. Plasmid construct was used as an internal control with suitable negative and water extraction controls. A total of 171 samples were found reactive by the Abbott AxSYM during the screening. Among these, 112 samples (Group A) were reactive by the second (Vironostika HIV Uni-Form II Ag/Ab) and third (HIV TRIDOT) assay as well and then declared as positive for HIV antibody. The remaining 59 samples showed discordant results in the first two assays. Among these 59 samples (Group B) one sample was negative by repeat testing (in duplicate) in Abbott AxSYM and declared negative and three more samples were declared negative by testing with two more third generation assays, Retrocheck (Qualpro Diagnsotics, Goa, India) and Genscreen HIV-1/2 (BIO-RAD, Marnes LA Coquette, France). When 32 available samples out of remaining 55 were tested for HIV-1 and HIV-2 RNA by real-time PCR, all except one were found negative. These 31 samples were declared negative for HIV. One plasma sample was found negative by Abbott AxSYM and hence not included for HIV RNA testing. For the remaining 23 individuals fresh plasma samples were not available. However original serum samples were available for 18 individuals and those samples were tested by one more fourth generation assay (Genscreen HIV Ag/Ab, BIORAD, Marnes LA Coquette, France) and a third generation assay (Retrocheck Qualpro Diagnsotics, Goa, India). All these 18 were found negative by three assays and declared negative. The number of samples tested by each test and their results are also shown in the Figure. The serological window period in HIV is considered to be four to six weeks. The assays that can detect p24 antigen along with antibodies can further reduce this time period. It is reported that the fourth generation HIV serological assays, compared to third generation assay, will reduce the diagnostic window period by further two to five days. [3] Currently, more and more laboratories in India have started using fourth generation assays routinely for HIV screening. Hence, it is important to know the in-use performance of these assays. As these assays are highly sensitive there is higher chance of false positive results. In our study it is found that the mean ± SD of the sample rate / cutoff rate of the group A ( n = 112) samples was 39. 44 ± 12.68 (range 7.1-71.82). All the samples except for two (98.2%) had an S/CO of> 10.00. The mean ± SD of the S/CO of the group B ( n = 58) samples was 1.91 ± 1.77 (range 0.9-11.97). All the 58 samples except one (98.3%) had an S/CO of less than 10, while for one of the samples it was 11.97. Calculating an arbitrary cut off of mean S/CO ± 3 SD of the 58 negative samples, the value would be 7.2. All the 58 samples except one (98.3%) had an S/CO of less than 7.2. Among the 170 repeatedly reactive samples by Abbot AxSYM system only 112 (67.5%) were found to be truly reactive for HIV. However, while taking the arbitrary cutoff of the S/CO value 7, among 113 samples 112 (99.1%) were positive for HIV. In this study we could not calculate the accuracy indices of the assays as the negative samples were not tested by any other gold standard assays like HIV-1 and 2 RNA due to financial constraints. Several HIV positive cases during the seroconversion period have been reported to be detected only by fourth generation assays or HIV RNA detection and these samples turn out to be negative by a variety of third generation assays. [4] Conversely, there are reports of third generation EIA showing similar sensitivity to fourth generation EIA (100%) and higher specificity (97.5 versus 95.1%). [5] In our study we were unable to identify any individual who was truly positive only by a fourth generation assay. Based on our findings we believe that any sample which shows an S/CO of < 7 may be a false positive result by the Abbot AxSYM system and can be declared negative by testing with two other fourth/third generation assays. However, any sample with> 7 S/CO should be considered as positive and if there is any discrepancy with other fourth generation assays it should be sent for molecular assay for the detection of HIV RNA. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08061f1.jpg] |
| |||||||||
{kind=link}