 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
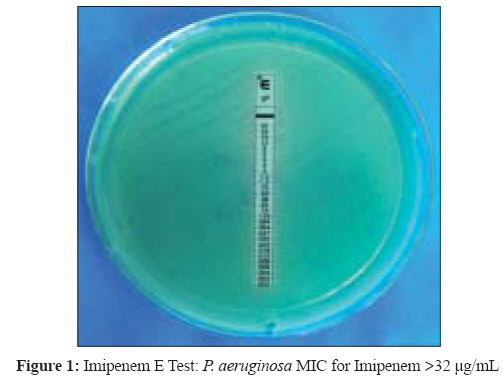
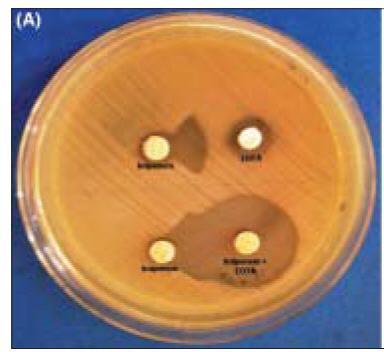
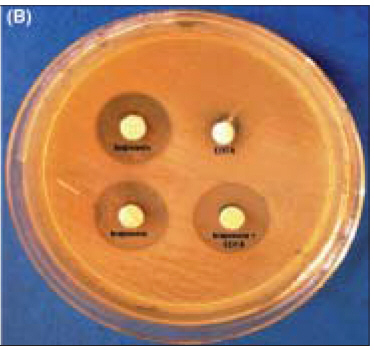
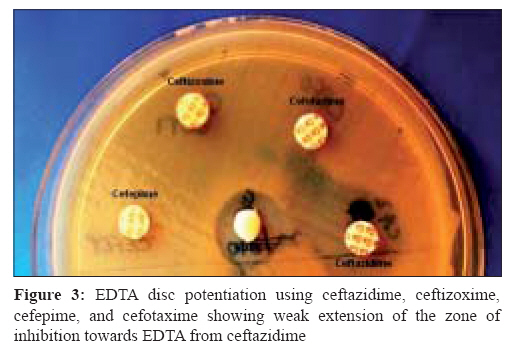
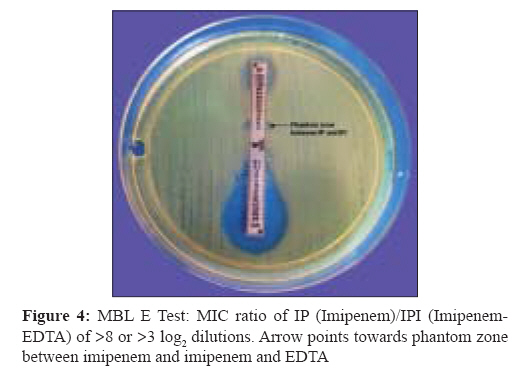
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 233-237 Original Article An evaluation of four different phenotypic techniques for detection of metallo-β-lactamase producing Pseudomonas aeruginosa Behera B, Mathur P, Das A, Kapil A, Sharma V Department of Laboratory Medicine, All India Institute of Medical Sciences, New Delhi - 110 029 Date of Submission: 02-Jan-2008 Code Number: mb08072 Abstract Purpose: The present study was undertaken to detect metallo-β-lactamase (MBL) in nosocomial isolates of Pseudomonas aeruginosa by four different phenotypic methods.Methods: Ninety-one consecutive P. aeruginosa isolates were subjected to susceptibility testing by disc-diffusion assay and Vitek 2. Imipenem resistance was determined by three different methods (disc-diffusion, Vitek 2 and E test). Screening for MBL production was done by imipenem-EDTA combined disc test, imipenem-EDTA double-disc synergy test, imipenem-EDTA MBL E test and EDTA disc potentiation using four cephalosporins. Results: Of 63 imipenem resistant isolates, MBL screening could be done in 56 isolates, of which 48 were MBL positive by combined disc test and 36 by the double disc synergy test. For confirmation of MBL production, MBL E test was done in 30 isolates. All the 30 isolates were confirmed to be MBL positive by the MBL E test method. EDTA disc potentiation using four cephalosporins was not very useful for MBL detection. Conclusions: Imipenem-EDTA combined disc test and imipenem-EDTA MBL E test are equally effective for MBL detection, but given the cost-constraints, combined disc test can be used as a convenient screening method in the clinical microbiology laboratory. Keywords: Carbapenem-imipenem, metallo-β-lactamase, Pseudomonas aeruginosa Pseudomonas aeruginosa is one of the most common pathogens causing nosocomial infections. Acquired drug resistance is frequent in nosocomial isolates of P. aeruginosa and often involves more than one antimicrobial class. Acquired metallo-β lactamases (MBL) have recently emerged as one of the most worrisome resistance mechanisms owing to their capacity to hydrolyze with the exception of aztreonam, all β-lactams including carbapenems and also because their genes are carried on highly mobile elements, allowing easy dissemination. [1] Such strains are not susceptible to therapeutic serine β lacatamase inhibitors (such as clavulanate and sulfones). [1] In recent years, MBL genes have spread from P. aeruginosa to members of Enterobacteriaceae. [2] MBL producing isolates are also associated with a higher morbidity and mortality. [1] Moreover, given that MBLs will hydrolyse virtually all classes of β-lactams and that we are several years away from the development of a safe therapeutic inhibitor; their continued spread would be a clinical disaster. [1] The occurrence of an MBL positive isolate in a hospital environment poses not only a therapeutic problem, but is also a serious concern for infection control management. With the global increase in the occurrence and types of MBLs, early detection is crucial; the benefits of which include timely implementation of strict infection control practices and treatment with alternative antimicrobials. [3] As a result of being difficult to detect, such organisms pose significant risks, particularly due to their role in unnoticed spread within institutions and their ability to participate in horizontal MBL gene transfer with other pathogens in the hospital. [3] Currently, no standardised method for MBL detection has been proposed and despite PCR being highly accurate and reliable, its accessibility is often limited to reference laboratories. [4] Several non molecular techniques have been studied, all taking advantage of the enzyme′s zinc dependence by using chelating agents, such as EDTA or 2 mercaptopropionic acid, to inhibit its activity. [4] Our institute, a tertiary care centre in India, has a very high prevalence of nosocomial infections due to P. aeruginosa . [5],[6] We have also found a very high prevalence of multidrug resistant (MDR) and ESBL positive gram negative bacteria in ICUs and other wards of our hospitals. [5],[6] Carbapenems and cephalosporin/inhibitor combinations are being used as "last resort" in these infections since the last few years. Therefore, we envisaged to ascertain the prevalence of MBL producing P. aeruginosa in our hospital in a setting of very high multi-drug resistance in this organism. Although a global increase in the prevalence of MBL producing P. aeruginosa has been reported, [1] limited data is available from our part of the world. Materials and Methods The study was conducted at the Department of Microbiology, All India Institute of Medical Sciences (AIIMS) and Department of Laboratory Medicine of its trauma centre. AIIMS is a 2500 bedded, tertiary care, referral and teaching hospital, where patients are referred from all over India. Bacterial isolates Antimicrobial susceptibility MBL screening Imipenem(IMP)-EDTA combined disc test Imipenem-EDTA double disc synergy test (DDST) EDTA disc potentiation using ceftazidime, ceftizoxime, cefepime and cefotaxime MBL E-test Results A total of 91 isolates of P. aeruginosa were included in the study. Of the 91 isolates of P. aeruginosa , 34 were isolated from bronchoalveolar lavage (BAL), 21 from blood, 14 from tracheal aspirate, 14 from pus, seven from urine, and one from CSF.Of the 91 isolates of Pseudomonas aeruginosa, 64 (70%) were resistant to ceftazidime, 68 (75%) to piperacillin, 54 (59%) to piperacilin/tazobactam, 58 (63%) to ticarcillin/clavulanic acid, 75 (82%) to cefoperazone, 67(74%) to amikacin, 74 (81%) to cefepime, 65 (71%) to levofloxacin, and 72 (79%) to ciprofloxacin by the disc diffusion (CLSI) method. The MIC of imipenem by E test was determined for all isolates giving discordant results between disk diffusion and Vitek 2. A total of 63 (69%) of isolates of P. aeruginosa were found to be resistant to imipenem. Of the 63-imipenem resistant isolates, 56 isolates were tested for MBL production. Forty-eight of these 56 isolates exhibited a ≥ 7 mm zone size enhancement in the combined disc test, whereas 36 isolates gave positive result by DDST. In the combined disc test, the mean ± S.D (95% confidence interval) zone augmentation values of the MBL positive and negative isolates were 15.67 ± 3.68 and 2.80 ± 2.13 mm respectively. The zone diameters were similar and reproducible when the procedure was repeated. Isolates, deemed MBL positive by DDST, were also shown to produce MBL by the combined disc test. MBL E test was done in 30 isolates (in 26 of which, both DDST and combined disc method demonstrated MBL production and four isolates were randomly selected from the 12 which gave a positive combined disc result and negative DDST result. In all these four strains, the MIC of imipenem + EDTA was 4 μg/mL and that of imipenem alone was> 256 μg/mL. Thus, all the 30 isolates were shown to be MBL positive by the MBL E test method. Phantom zone between IP/IPI was noted in 5 isolates. EDTA disc potentiation with four cephalosporins. (ceftazidime, ceftizoxime, cefepime, cefotaxime) was done in 30 isolates. In none of the 30 isolates, zone enhancement towards EDTA disc was observed with cefotaxime, cefepime or ceftizoxime disc. A very small zone enhancement towards EDTA disc was seen in five isolates. Therefore, we did not use these discs for the remaining isolates. Discussion Carbapenems are β-lactam antibiotics, presently considered as the most potent agents of treatment of multidrug resistant gram negative bacterial infections due to the stability of these agents against the majority of β-lactamases and their high rate of permeation through bacterial outer membranes. However, in the last decade there have been increasing reports of resistance to this life-saving antimicrobial in Pseudomonas aeruginosa . [6] Resistance to carbapenems in P.aeruginosa may develop due to impermeability, which occurs due to the loss of the opr D porin, the up regulation of an active efflux system present in these organisms, or the production of MBLs. [3] Carbapenem hydrolysing MBLs have been reported in several countries and have emerged as the most important mechanism of carbapenem resistance. [3],[14] Production of MBL by Pseudomonas spp. and other gram negative bacteria has tremendous therapeutic consequences, since these organisms also carry other multidrug resistance genes and the only viable treatment option remains the potentially toxic polymyxin B and colistin. [15] Since there is no standard guideline for detection of MBL, different studies have reported the use of different methods. MBL production has been previously reported from India. [16],[17],[18],[19],[20] Most studies have used IPM-EDTA combined disc, double disc synergy test using IPM-EDTA and modified Hodge test. According to those studies MBL production in P. aeruginosa ranged from 7%-65%. [16-20] In this study, we have used four different methods of screening for MBL production. With the Imipenem and EDTA combined disc test with a cut-off> 7 mm, the positive and negative results were more clearly discriminated. One of the major disadvantages of DDST was the subjective interpretation of result in some instances. The combined disc method using imipenem + EDTA was found to be superior to DDST (using imipenem - EDTA) and EDTA disc potentiation with ceftazidime, cefotaxime, ceftizoxime, cefepime. This is in accordance with other published studies, which have found the combined disc method to be one of the most sensitive techniques for detecting MBL. [21] We also found the MBL E test to be very sensitive for detection of MBL on P. aeruginosa. There are conflicting reports regarding the performance of MBL E test in the literature. [21] MBL E - Test has been reported to be insensitive to detect carbapenem sensitive MBL carrying organisms. [21] In our study, we screened only carbapenem resistant isolates with MBL E -Test, which may have accounted for very high sensitivity of the test. We found that all 26 isolates found to be MBL positive by combined disc were also positive with the E test and four, which were positive by the combined and negative by DDST were found to be MBL positive by E test. The E test MBL strip, based on a combination of a β lactam substrate and a β lactam/ metallo β lactamase inhibitor is specifically designed to detect as many clinically relevant MBL as possible. [13] The E test MBL strip (IP-IPE) has the ability to detect metallo β lactamases, both chromosomally and plasmid mediated, in aerobic and anaerobic bacteria. [13] This novel method could be used by clinical laboratories to monitor the emergence of metallo β lactamase in a range of clinically significant bacteria and by surveillance network to establish the spread of the enzyme. Both combined disc and E test were found to be equally sensitive for MBL detection. However, given the cost constraints of E test, a simple screening method like combined imipenem/imipenem + EDTA method can be used.The technique is very easy, economical and can be incorporated into the routine testing of any busy Microbiology laboratory, as has been done for ESBL screening. The unique problem with MBLs is their unrivalled broad-spectrum resistance profile. In addition, in many cases the MBL genes may be located on plasmids with genes encoding other antibiotic resistance determinants i.e., aminoglycosides resistance genes. These MBL positive strains are usually resistant to β lactams, aminoglycosides and fluoroquinolones. However, they usually remain sensitive to polymyxin. In our study, we found all the isolates, except for six to be susceptible to polymyxin B (300 units; Sigma-Aldrich, USA, Unpublished data). The correlation between carriage of MBL genes and carbapenem resistance is often imperfect. Two speculations have been proposed to explain this imperfect correlation. Either MBL genes are not always expressed or substantive resistance may require uptake of carbapenems as well as presence of MBLs. With the emergence of carbapenem sensitive MBL carrying organisms, the issue of which isolates to select for phenotypic MBL detection, is controversial. In our experience, the combined disc method can be applied on all isolates. Screening only carbapenem resistant organisms is most often preferred, but is suboptimal. It is also debated that screening all isolates will unnecessarily increase the workload with a lower yield. Thus, laboratories can select those strains, which show resistance to ceftazidime and ticarcillin-clavulanic acid. Although some authors recommend using a ceftazidime disc instead of imipenem disc for combined disc/DDST, [12] MBL producing organisms may have other ceftazidime resistance mechanisms. With such strains, combined disc/DDST using ceftazidime will not show MBL production and therefore, imipenem disc must be used for screening of MBL. To conclude, our study found imipenem-EDTA combined disc test and imipenem-EDTA MBL E test to be equally effective for MBL detection, however, we believe that given the cost-constraints, combined disc test could be used as a convenient screening method in the clinical microbiology laboratories. These laboratories must evaluate the various screening methods for detection of MBL in order to correctly report this important mechanism of antimicrobial resistance. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08072f2a.jpg] [mb08072f2a&b.jpg] [mb08072f1.jpg] [mb08072f3.jpg] [mb08072f4.jpg] [mb08072f2b.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}