 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
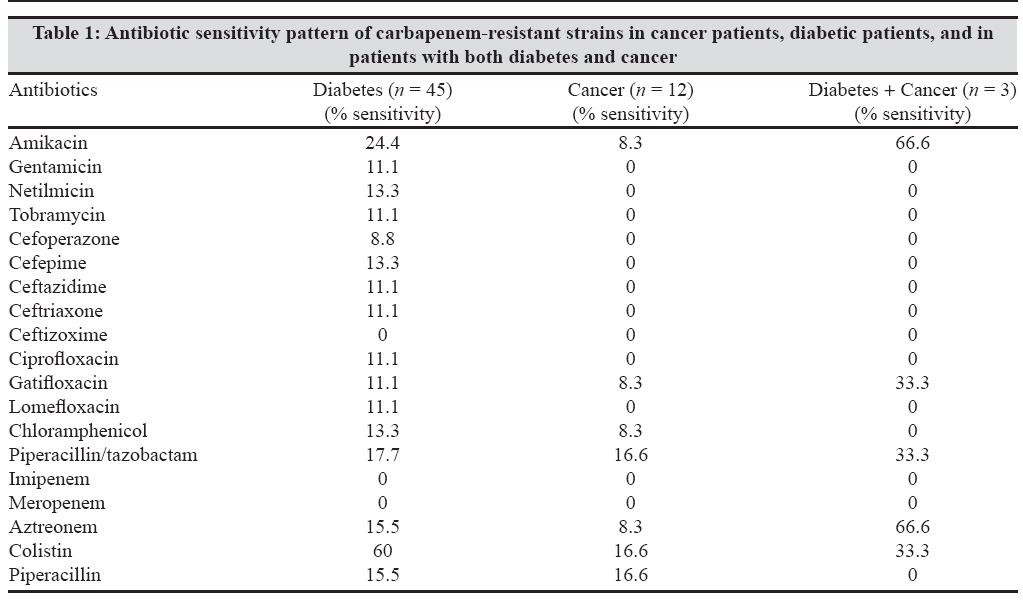
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 238-240 Brief Communication Incidence of carbapenem-resistant Pseudomonas aeruginosa in diabetes and cancer patients Varaiya A, Kulkarni M, Bhalekar P, Dogra J Department of Microbiology, SL Raheja Hospital, Mumbai - 400 016, Maharashtra Date of Submission: 21-Jun-2007 Code Number: mb08073 Abstract Two hundred and thirty isolates of Pseudomonas aeruginosa were obtained from samples of patients having diabetes (75%), cancer (20%), and both diabetes and cancer (5%) who were admitted to a tertiary care hospital in Western India from January to December 2006. These isolates were tested for susceptibility to antipseudomonal drugs and considered to be resistant to carbapenem when the zone of inhibition around imipenem and meropenem discs was ≤13 mm. Of these 230 isolates, 26% were found to be carbapenem resistant. The rapid dissemination of carbapenem resistance is worrisome and calls for the implementation of surveillance studies as well as judicious use of antibiotics.Keywords: Carbapenem resistance, metallo β-lactamase, pseudomonas aeruginosa Multiple factors contribute to make Pseudomonas aeruginosa a nosocomial pathogen, for example, injudicious administration of broad-spectrum antibiotics, instrumentation, and intrinsic resistance of microorganisms to numerous antimicrobial agents. [1] The introduction of carbapenems into clinical practice was of great help in the treatment of serious bacterial infections caused by β-lactam-resistant bacteria. Carbapenems, due to their stability to hydrolysis by most β-lactamases, have been the drugs of choice for treatment of infections caused by penicillin-resistant or cephalosporin-resistant gram-negative infections. [2] In view of the paucity of information on carbapenem-resistant P. aeruginosa infections in diabetes and cancer patients, we undertook the present study to determine its incidence and also to find out the clinical outcome in such patients admitted to a tertiary care hospital in western India. Materials and Methods Over a one year period from January to December 2006, 230 isolates of P. aeruginosa were obtained from diabetic and cancer patients admitted to the hospital. The specimens were collected, transported, and processed in the laboratory without any delay. They included tissue from nonhealing ulcers (78), respiratory secretions (73), urine (34), pus/wound swabs (32), blood (5), bile (4), and sterile body fluids (4).The isolates were identified by standard laboratory techniques. [3] Blood cultures were processed using an automated method with Versa TREK (Trivitron). Antimicrobial sensitivity testing was performed on Mueller-Hinton agar plates with commercially available discs (Hi-Media, Mumbai) by the Kirby-Bauer disc diffusion method. The results were recorded and interpreted as per CLSI recommendations. [4] P. aeruginosa ATCC 27853 was used as the negative control. The routine antibiotic sensitivity tests were put up for amikacin (30 μg), gentamicin (10 μg), netilmicin (30 μg), tobramycin (10 μg), cefoperazone (75 μg), cefepime (30 μg), ceftazidime (30 μg), ceftriaxone (30 μg), ceftizoxime (30 μg), ciprofloxacin (5 μg), gatifloxacin (5 μg), lomefloxacin (10 μg), imipenem (10 μg), meropenem (10 μg), chloramphenicol (30 μg), piperacillin/tazobactam (100/10 μg), aztreonem (30 μg), and colistin (10 μg). Isolates were considered to be carbapenem resistant when the zone of inhibition around imipenem and meropenem discs was ≤13 mm. Results Of the 230 isolates of P. aeruginosa , 60 (26%) were found to be resistant to carbapenems. Of these 60 isolates, 45 (75%) were from diabetic patients and 12 (20%) were from cancer patients; the cancer cases included carcinoma of the oesophagus (4), haematolymphoid malignancies with febrile neutropenia (3), carcinoma of the lung (2), carcinoma of the pancreas (1), carcinoma of the rectum (1) and carcinoma of the prostrate (1). Three (5%) patients had both diabetes and oesophageal cancer. Forty patients (66.6%) were males and 20 (33.3%) were females; the mean age was 62 years (range 37-87 years).Overall microbial sensitivity to the different antibiotics was as follows: colistin 48%, amikacin 23%, gatifloxacin 28%, piperacillin/tazobactam 18%, piperacillin 15%, and aztreonam 10%. The antibiotic sensitivity of carbapenem-resistant strains in patients with diabetes, cancer, and having both diabetes and cancer is shown in [Table - 1]. Of the 60 patients who had carbapenem-resistant P aeruginosa , nine patients died. The causes of death were chronic renal failure (5), terminal respiratory arrest due to septicaemia (3), and septicaemia with progressive metastatic carcinoma (1). Among the 51 patients who survived, 8 (15.6%) needed readmission to the hospital. The mean hospital stay of patients was 25 days (range 6-44 days). Discussion Carbapenems are used for treating serious infections caused by multidrug-resistant gram-negative bacilli. Resistance to carbapenem is due to decreased outer membrane permeability, increased efflux systems, alteration of penicillin-binding proteins, and the production of carbapenem hydrolyzing enzymes, i.e., carbapenemases. The resistance may also be due to the production of metallo-β-lactamases (MBL); such resistance can be chromosomally encoded or plasmid mediated. [5] In various studies across the world, varying rates of resistance (4-60%) have been reported for imipenem and meropenem. [6] Of the Indian workers, Gladstone et al reported 42.8% carbapenem resistance among P. aeruginosa isolates, [5] whereas Taneja et al reported that 36.4% of nosocomial urinary tract infections were caused by nonfermenters resistant to imipenem. [7] In the present study, of the 230 P. aeruginosa isolates, we found that 26% were resistant to both imipenem and meropenem. In this study, the detection of carbapenem resistance in P. aeruginosa was done by the Kirby-Bauer disc diffusion method. However, further screening for detection and confirmation of MBL production should be done by the modified Hodge test, the modified imipenem-EDTA double-disc synergy test, or the E test. [2] In diabetic patients, foot infections are frequent; these infections are polymicrobial and there is a high incidence of multidrug-resistant P. aeruginosa reported from patients with type 2 diabetes mellitus. [8] We found 75% resistance to carbapenem amongst the P. aeruginosa isolates from such cases. Amongst the cancer patients, Maschmeyer et al reported that, overall, 5-12% patients had infection with P. aeruginosa , while the incidence was 1-2.5% in patients with febrile neutropenia. [9] In our study, 20% of the cancer patients had carbapenem-resistant P. aeruginosa infection, while the incidence was 5% in patients having haematolymphoid malignancy with febrile neutropenia. P. aeruginosa is responsible for 3-7% of bloodstream infections and high mortality rates (27-48%) in critically ill patients. [10] We found that 8.3% of bloodstream infections were due to P. aeruginosa and there was a 15% mortality in ICU patients. Polymyxin B or colistin represent the best treatment options. [11] However, colistin is very expensive and this limits its use. Our patients were treated with a combination of gatifloxacin, amikacin, and piperacillin/tazobactam. Of the 51 patients who survived, 8 (15.6%) needed readmission to the hospital: seven were diabetic patients admitted with either nonhealing wounds or urinary tract infections and one was a cancer patient admitted because of deterioration in his clinical condition due to progressive disease. In conclusion, our study highlights increasing resistance in P. aeruginosa towards imipenem and meropenem. This rapid dissemination of carbapenem resistance is worrisome and calls for the implementation of surveillance studies and the judicious selection of antibiotics in clinical practice. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08073t1.jpg] |
| |||||||||
{kind=link}