 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
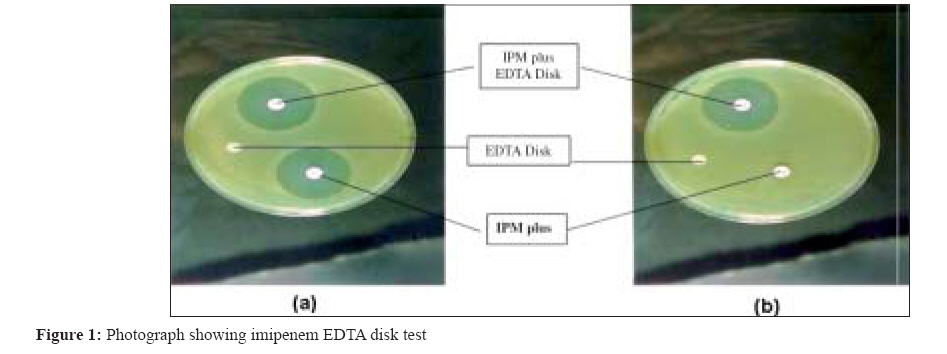
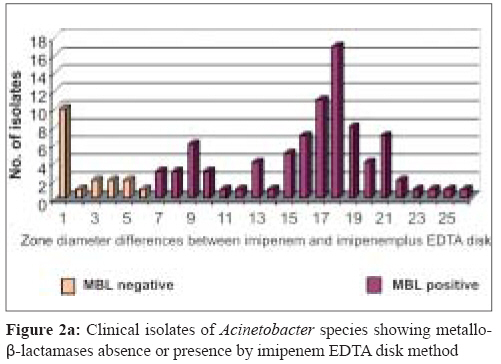
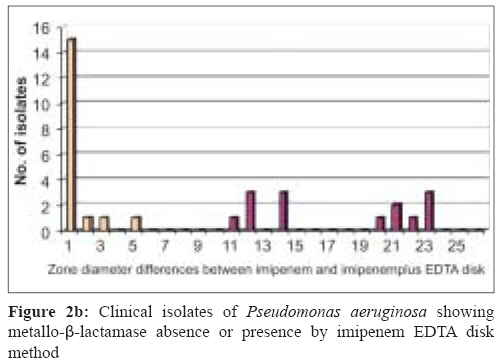
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 243-245 Brief Communication Metallo-β-lactamase-producing clinical isolates of Acinetobacter species and Pseudomonas aeruginosa from intensive care unit patients of a tertiary care hospital Irfan S, Zafar A, Guhar D, Ahsan T, Hasan R Clinical Laboratory, Department of Pathology and Microbiology, Aga Khan University and Hospital, Stadium Road, Karachi Date of Submission: 03-May-2007 Code Number: mb08075 Abstract Prompt detection of metallo-β-lactamase (MBL) producing isolates is necessary to prevent their dissemination. Frequency of MBLs producing strains among multidrug resistant (MDR) Acinetobacter species and Pseudomonas aeruginosa was evaluated in critical care patients using imipenem-EDTA disk method. One hundred MDR Acinetobacter spp. and 42 Pseudomonas aeruginosa were checked for MBL production, from January to June 2001. MBL was produced by 96.6 % of imipenem-resistant Acinetobacter isolates, whereas 100% imipenem-resistant Pseudomonas aeroginosa isolates were MBL producers. Carbapenem resistance in MDR Acinetobacter spp. and Pseudomonas aeruginosa isolates in this study was due to MBLs. This calls for strict infection control measures to prevent further dissemination.Keywords: Acinetobacter spp, metallo-β-lactamase, Pseudomonas aeruginosa Carbapenem group of antibiotics play a vital role in the management of hospital-acquired gram negative infections, because of their broad spectrum activity and stability to hydrolysis by most of the β-lactamases, including extended spectrum β-lactamases (ESBLs). Nosocomial outbreaks of carbapenem-resistant Pseudomonas aeruginosa and Acinetobacter spp. due to metallo-β-lactamases (MBLs) production have been reported from different regions. [1],[2],[3] The emergence of these MBLs in gram negative bacilli is becoming a therapeutic challenge as these enzymes possess high hydrolytic activity that leads to degradation of higher generation cephalosporins. Moreover, the treatment alternatives are unavailable, or expensive/toxic with poor outcome. [4] Plasmid mediated MBL genes spread rapidly to other species of gram negative bacilli; [5] therefore rapid detection of metallo-β-lactamases production is necessary to modify therapy and to initiate effective infection control to prevent their dissemination. To date there has been one report from Pakistan suggesting presence of MBL producing isolate. [6] There is however need for a systematic study to assess the extent of this form of resistance amongst our isolates. The purpose of this study was to evaluate the metallo-β-lactamase (MBL) production among multidrug resistant (MDR) Acinetobacter spp. and Pseudomonas aeruginosa , isolated from clinical specimens of intensive care unit patients. Materials and Methods This study was conducted in the clinical microbiology laboratory of The Aga Khan University Hospital, Karachi, Pakistan. One hundred MDR clinical isolates of Acinetobacter species and 42 Pseudomonas aeruginosa were studied for MBL production. These organisms were isolated from respiratory secretions, wound swabs, urine and blood culture specimens of intensive care unit patients, admitted from January to April 2001. A multidrug resistant isolate was defined as resistance to two or more drugs or drug classes of therapeutic relevance. [7] All the isolates of Pseudomonas aeruginosa were characterised to species level using standard procedures. Similarly, Acinetobacter isolates were characterised to the genus level using these procedures. Susceptibility testing against CLSI (Clinical Laboratory Standards institute) recommended antibiotics were performed by Kirby Bauer disk diffusion method. [8] The antibiotic susceptibility was further confirmed by determining the minimum inhibitory concentration on agar dilution method as recommended by CLSI. E. coli ATCC 25922 and P. aeruginosa ATCC 27853 were used as control strains. The organisms were considered as susceptible to imipenem if MIC was < 4 μg/mL and resistant if MIC was ≥16 μg/mL.[8] To identify MBL production in these isolates, we used IPM-EDTA-disk synergy test developed by Yong D et al . [9] To make 0.5 M EDTA solution 186.1 g of disodium EDTA was dissolved in 1000 mL of distilled water and pH was adjusted to 8.0 by using NaOH. The mixture was then sterilised by autoclaving. EDTA imipenem disks were prepared by adding EDTA solution to 10-μg-imipenem disks to obtain a concentration of 750 μg. The disks were dried immediately in an incubator and stored at 4°C or at −20°C in an air tight vial without desiccant. Test strains were adjusted to the McFarland 0.5 standard and were inoculated to Mueller Hinton agar. A 10-μg-imipenem disk and an imipenem plus 750 μg EDTA were placed on Mueller Hinton agar. Another disk containing only 750 μg EDTA was also placed as a control. After overnight incubation, the established zone diameter difference of ≥ 7 mm between imipenem disk and imipenem plus EDTA was interpreted as EDTA synergy positive. [Figure - 1] shows a negative imipenem plus EDTA disk test for ATCC strains of Pseudomonas aeruginosa and positive for MBL producing clinical isolate of Pseudomonas aeruginosa . Results Imipenem-resistance by disc diffusion method was found in 90 out of 100 isolates of Acinetobacter spp. Of the 90 imipenem-resistant Acinetobacter spp. 83(96.6%) were metallo-β-lactamase producers. Whereas, remaining 17 isolates, including the 10 imipenem-sensitive isolates, did not show evidence of metallo-β-lactamase production. The average zone diameter difference between imipenem disk and imipenem plus EDTA disk for MBL-positive isolates was 16 mm [Figure 2a]. Among 42 Pseudomonas aeruginosa isolates, 25 showed resistance against imipenem by disc diffusion method. Imipenem-EDTA disk method showed 100% metallo-β-lactamase production in imipenem resistant Pseudomonas aeruginosa isolates with an average difference of 14 mm in zone diameter between imipenem disk and imipenem plus EDTA disk for MBL-positive isolates. Imipenem sensitive group did not show any metallo-β-lactamase producing isolate [Figure 2b]. Discussion By using the Imipenem-EDTA disk method, a very high percentage of imipenem resistant Acinetobacter spp. (97%) and Pseudomonas aeruginosa (100%) isolates showed metallo-β-lactamase activity. This finding is consistent with reports from other tertiary care hospitals, [10] giving the evidence that acquired MBLs can rapidly emerge and establish a condition of endemicity in certain epidemiological settings. A majority of our isolates also showed resistance to other important groups of antibiotics including third generation cephalosporin, aminoglycoside and quinolone, which is a characteristic of majority of metallo-β-lactamases producing isolates. [11] A number of MBLs producers in both organisms showed significant difference between zone of inhibition by imipenem and imipenem plus EDTA disk. When compared with non-MBL producers the average zone difference for the MBL producers was 15 mm versus 2 mm for the non-MBL producers, thus making this test reliable for initial screening of the MBL production in clinical isolates. Reports from various parts of the world showing emergence of metallo-β-lactamase enzymes in Enterobacteriaceae [5] is an evidence for the spread of these enzymes in this family. Emergence of MBLs producing Acinetobacter spp. and Pseudomonas aeruginosa in our clinical strains is alarming and reflects excessive use of carbapenem. Therefore, early detection and prompt instillation of infection control measures is important to prevent further spread of MBLs to other gram negative rods. Additionally, it is also important to follow antibiotic restriction policies to avoid excessive use of carbapenem and other broad spectrum antibiotics. Finally, to understand the epidemiology, there is a need of genetic analysis and also the typing of metallo-β-lactamase enzymes. In conclusion, by using imipenem-EDTA disk method as a screening test for metallo-β-lactamase production, we found a very high percentage of metallo-β-lactamase producing isolates among multidrug resistant Acinetobacter spp. and Pseudomonas aeruginosa isolates. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08075f2b.jpg] [mb08075f2a.jpg] [mb08075f1a.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}