 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
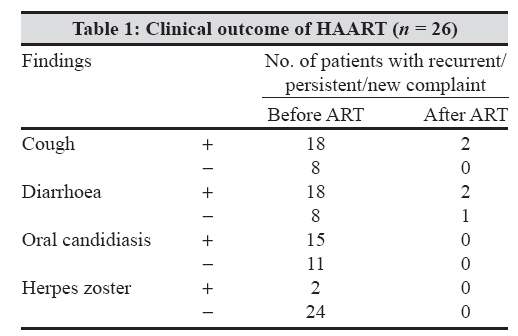
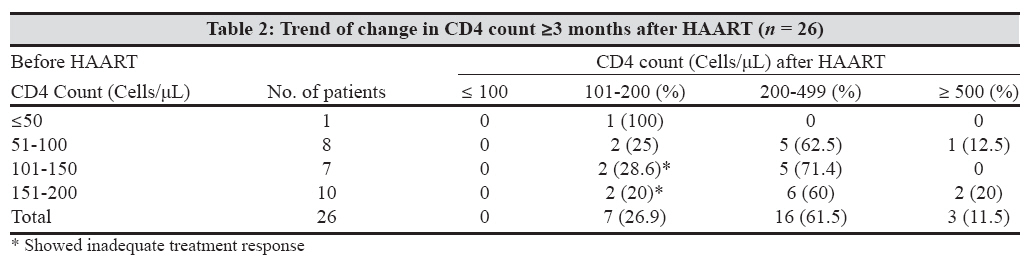
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 256-258 Brief Communication Correlation between baseline CD4 + T-Lymphocyte count and plasma viral load in AIDS patients and their early clinical and immunological response to HAART: A preliminary study Gautam H, Bhalla P, Saini S, Dewan R Department of Microbiology, Maulana Azad Medical College, New Delhi - 110 002 Date of Submission: 31-Jul-2007 Code Number: mb08079 Abstract The aim of this study was to determine the clinical, immunological and virological status of newly diagnosed AIDS cases and to monitor their clinical and immunological response to HAART after a minimum period of three months. Forty three drug naive AIDS patients were enrolled. The most common presenting complaints were weight loss (74.4%), cough (72.1%) and diarrhoea (67.4%). Mean baseline CD4 cell count was 112 ± 60 cells/μL and mean baseline plasma viral load of 31 patients studied was 192,686 copies/mL. Baseline plasma viral load was higher among patients with lower baseline CD4 cell count. During follow-up, 80.8% patients showed clinical improvement, while a CD4 cell count increased by ≥50 cells/μL in 84.6% cases. Mean CD4 cell count increased from 126 ± 16.6 cells/μL at baseline to 278 ± 196.7 cells/μL.Keywords: CD4+ T-lymphocytes, HAART, plasma viral load Over the past decade, HIV/AIDS has become a major public health problem in India. [1] Anti-retroviral therapy (ART) clinics were started in 2004 by the Govt. of India, however, there are very few published reports regarding the efficacy of the highly active anti-retroviral therapy (HAART) regimens that are being used in India, based on monitoring of clinical and immunological response. [2],[3] As per WHO and CDC guidelines, a CD4 count of < 200 cells/μL should be used for the initiation of ART. In the absence of a CD4 cell count, a total lymphocyte count below 1200 cells/mm3 in patients with symptomatic HIV disease has been recommended as a guide to the initiation of ART. [4],[5] With higher CD4 cell counts, HIV RNA level of above 50,000-1,00,000 copies/mL can be used for initiation of therapy. [6] While monitoring response to ART, decreasing frequency of opportunistic infection(s) is an important sign of good clinical response [1] and CD4 cell count typically increases 100-150 cells/mm 3 /year with an accelerated response in the first three months. [7] HIV viral load measurement, which may detect treatment failure earlier than immunological and clinical assessment, is currently not recommended in resource-limited settings. [4] In view of the above, a pilot study was undertaken to determine the clinical profile, immunological and virological status of newly diagnosed HIV seropositive patients and to monitor their early clinical and immunological response to HAART. Materials and Methods Forty three drug naive AIDS patients attending the ART clinic at Lok Nayak Hospital, New Delhi, India, were studied from February to November 2006. Clinical staging of the disease was done according to WHO guidelines. [4] At recruitment, blood sample was taken from all patients, in plain vial for serum (HIV testing) and in K3EDTA vacutainer for whole blood (CD4 cell count) and plasma (viral load determination) after obtaining informed consent. Serum and plasma were separated on the same day and if not tested, were kept at −70° C until analysis. Serodiagnosis of HIV infection was made by three ELISA/Rapid tests. The total lymphocyte count (TLC) was performed by automated cell counter (MS9-3H, Melet Schloesing Laboratories) while absolute count of CD4+ T-lymphocytes was determined by flow cytometry using FACSCount TM system (Becton Dickinson). Plasma viral load (PVL) was estimated using AMPLICOR HIV-1 MONITOR test, version 1.5 (Roche Diagnostics) with a linear dynamic range of 400-750,000 copies/mL. TLC could be determined for 37 out of 43 cases recruited. Baseline PVL could be determined for 31 out of 43 cases recruited but could not be done at follow-up due to non-availability of kit and reagents. All cases in the study were started on HAART as per NACO guidelines. [1] Patients were asked to report to follow-up after a minimum period of three months to monitor the clinical and immunological response to HAART. On follow-up, the cases were categorised as clinical failure and immunological failure as per WHO guidelines. [4] CD4 cell count typically increases by> 50 cells/μL at four to eight weeks and an additional 50 to 100 cells/μL/year thereafter.[6] For quantitative data, difference between the mean was analysed by Wilcoxon sign rank test and unpaired data by Mann Whitney test while for qualitative data, proportions between the groups was compared by Chi-square test. Results All patients studied had a baseline CD4 cell count ranging from 7-195 cells/μL (mean 112 ± 60 cells/μL). CD4 cell count of < 50 cells/μL was seen in 18.6% patients signifying the stage of severe immunosuppression. Seventy two percent patients had a total lymphocyte count (TLC) ≤1200/mm 3 and 83% patients had CD4:CD8 ratio ≤0.2. The CD4 percentage was < 14 percent in 89.2% cases. The baseline plasma viral load (PVL) of 31 patients studied ranged from 1607-> 750000 copies/mL with a mean of 192,686 copies/mL. PVL was higher among patients with lower CD4 cell count as all patients with CD4 cell count ≤50 cells/μL had PVL> 100000 copies/mL. The most common presenting complaints in the patients studied were weight loss (74.4%), cough (72.1%) and diarrhoea (67.4%). Twenty one percent patients belonged to WHO clinical stage IV (mean CD4 cell count = 74.6 cells/μL), 51% to stage III (mean CD4 cell count = 103.9 cells/μL) and 28% to stage II (mean CD4 cell count = 155 cells/μL). Adherence to HAART was> 95% in the patients studied. Out of 43 patients, eight patients (19%) expired before reporting for follow-up and nine patients(21%) did not report for follow-up. Twenty six patients (60%) came for follow-up after a mean period of 4.7 months (range = 3 to 6 months). All patients who expired had a CD4 cell count between 7-69 cells/μL (mean 34.5 cells/μL) while PVL ranged from 1,67,739 -> 7,50,000 copies/mL (mean 4,24,548 copies/mL). Out of the 26 patients who came for follow-up, 21 patients (80.8%) showed clinical improvement, while clinical failure was suspected in five patients (19.2%) as seen in [Table - 1]. All patients who expired had a CD4 cell count between 7-69 cells/μL (mean 35.4 cell cells/μL) while PVL ranged from 1,67,739 - > 7,50,000 copies/mL(mean 4,24,548 copies/mL). Out of the 26 patients who came for follow-up, 21 patients (80.8%) showed cliniccal improvment, while clinical failure was suspected in five patients (19.2%) as seen in table 1. [Table - 2] shows the change in CD4 count after ≥3 months of HAART. All except four patients (15.4%) showed an increase of ≥50 CD4 cells/μL. Among these four cases, three also showed a clinical failure. In our study, mean CD4 cell count of patients who came for follow-up increased from 126 ± 16.6 cells/μL (median130 cells/μL) at baseline to 278 ± 196.7 cells/μL(median 238 cells/μL) (P < 0.001), mean total lymphocyte count (TLC) increased from 1621 ± 780.7/mm 3 (median 1200/mm 3 ) at baseline to 2491 ± 1242.4/mm 3 (median 2000/mm 3 ) ( P < 0.05). Among the patients who expired (8) and those who were alive at follow-up (26), a significant difference ( P < 0.001) was found between the baseline mean CD4 cell count (35 cells/μL vs 126 cells/μL), mean CD4% (3.7 vs 8.3), mean PVL (4,24,548 copies/mL vs 1,45,766 copies/mL) and mean TLC (700 mm 3 vs 1621 mm 3 ). Discussion As per NACO guidelines, currently in India, absolute CD4 cell count is being used as the basis for initiation of ART. [1] The validity of this approach in comparison to plasma viral load has not been studied widely in India. Baseline plasma viral load estimates are being carried out in very few patients because of limited resources. The present study was undertaken as a pilot study for this purpose. In the present study, baseline mean CD4 cell count was 112.1 ± 60.29 cells/μL and mean CD4:CD8 ratio was 0.14 ± 0.09 which is in agreement with studies among similar patient groups from other parts of India. [8],[9],[10] CDC has expanded the AIDS surveillance case definition to include all HIV-infected persons with CD4+ T-lymphocyte counts of less than 200 cells/μL or a CD4+ percentage of less than 14. [5] In our study, the CD4 percentage was < 14 in 89.2% cases with CD4 count < 200 cells/μL. In a study from the US, it is said that CD4 absolute count is the best predictor of an adverse event when the CD4 count is ≤200 cells/uL while CD4+ percentage is a better predictor when the CD4 count is ≥200 cells/µL. [11] In our study, at baseline, 70.3% patients had a total lymphocyte count (TLC) ≤1200/mm 3 which is in contrast with one study in Mozambique, in which the sensitivity of TLC to detect the cases with CD4 count < 200 cells/μL was only 48.9%.[12] However, a study from U.K showed that TLC is almost as reliable as CD4 count for prediction of AIDS defining opportunistic infections. [13] The threshold value for the dichotomisation of TLC was taken as 1200 cells/mm 3 , considered a marker of serious immunosuppression according to WHO for resource limited settings. [4] Eighty four pecent cases showed an increase of more than 50 cells/μL following HAART which is in concordance with another recent Indian study. [2] Our study showed a mean CD4 gain of 152 cells/μL within a mean duration of 4.7 months. However, another Indian study from Chennai has documented a mean CD4 gain of 188 cells/μL within a mean duration of 4.3 months. [3] A statistically significant increase in the mean TLC was also observed by us, which is in accordance with another study which showed that within the first two years of HAART, the direction of change in TLC appears to be concomitant with changes in CD4 count. [8] In conclusion, good treatment response to the HAART regimens being provided was observed in> 80% patients, implying that the HAART is efficacious and its efficacy would further increase if it will be given well in time, since initiation of therapy at an advanced stage of immunosuppression (≤50 cells/μL) may not be as effective. Those patients, who expired after the initiation of HAART, showed statistically significant lower baseline values of mean CD4 cell count, mean CD4+ percentage, mean total lymphocyte count and higher baseline value of mean HIV plasma viral load in comparison to the patients who were alive at follow-up. In places where CD4 count facilities are not available, total lymphocyte count ≤1200/mm 3 may be used as a surrogate marker of CD4 cell count < 200/μL, however, further studies are required in HIV patients with CD4 count 200-499/μL and ≥ 500/μL References
Copyright 2008 - Indian Journal of Medical Microbiology Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 256-258 Brief Communication Correlation between baseline CD4 + T-Lymphocyte count and plasma viral load in AIDS patients and their early clinical and immunological response to HAART: A preliminary study Gautam H, Bhalla P, Saini S, Dewan R Department of Microbiology, Maulana Azad Medical College, New Delhi - 110 002 Date of Submission: 31-Jul-2007 Code Number: mb08079 Abstract The aim of this study was to determine the clinical, immunological and virological status of newly diagnosed AIDS cases and to monitor their clinical and immunological response to HAART after a minimum period of three months. Forty three drug naive AIDS patients were enrolled. The most common presenting complaints were weight loss (74.4%), cough (72.1%) and diarrhoea (67.4%). Mean baseline CD4 cell count was 112 ± 60 cells/μL and mean baseline plasma viral load of 31 patients studied was 192,686 copies/mL. Baseline plasma viral load was higher among patients with lower baseline CD4 cell count. During follow-up, 80.8% patients showed clinical improvement, while a CD4 cell count increased by ≥50 cells/μL in 84.6% cases. Mean CD4 cell count increased from 126 ± 16.6 cells/μL at baseline to 278 ± 196.7 cells/μL.Keywords: CD4+ T-lymphocytes, HAART, plasma viral load Over the past decade, HIV/AIDS has become a major public health problem in India. [1] Anti-retroviral therapy (ART) clinics were started in 2004 by the Govt. of India, however, there are very few published reports regarding the efficacy of the highly active anti-retroviral therapy (HAART) regimens that are being used in India, based on monitoring of clinical and immunological response. [2],[3] As per WHO and CDC guidelines, a CD4 count of < 200 cells/μL should be used for the initiation of ART. In the absence of a CD4 cell count, a total lymphocyte count below 1200 cells/mm3 in patients with symptomatic HIV disease has been recommended as a guide to the initiation of ART. [4],[5] With higher CD4 cell counts, HIV RNA level of above 50,000-1,00,000 copies/mL can be used for initiation of therapy. [6] While monitoring response to ART, decreasing frequency of opportunistic infection(s) is an important sign of good clinical response [1] and CD4 cell count typically increases 100-150 cells/mm 3 /year with an accelerated response in the first three months. [7] HIV viral load measurement, which may detect treatment failure earlier than immunological and clinical assessment, is currently not recommended in resource-limited settings. [4] In view of the above, a pilot study was undertaken to determine the clinical profile, immunological and virological status of newly diagnosed HIV seropositive patients and to monitor their early clinical and immunological response to HAART. Materials and Methods Forty three drug naive AIDS patients attending the ART clinic at Lok Nayak Hospital, New Delhi, India, were studied from February to November 2006. Clinical staging of the disease was done according to WHO guidelines. [4] At recruitment, blood sample was taken from all patients, in plain vial for serum (HIV testing) and in K3EDTA vacutainer for whole blood (CD4 cell count) and plasma (viral load determination) after obtaining informed consent. Serum and plasma were separated on the same day and if not tested, were kept at −70° C until analysis. Serodiagnosis of HIV infection was made by three ELISA/Rapid tests. The total lymphocyte count (TLC) was performed by automated cell counter (MS9-3H, Melet Schloesing Laboratories) while absolute count of CD4+ T-lymphocytes was determined by flow cytometry using FACSCount TM system (Becton Dickinson). Plasma viral load (PVL) was estimated using AMPLICOR HIV-1 MONITOR test, version 1.5 (Roche Diagnostics) with a linear dynamic range of 400-750,000 copies/mL. TLC could be determined for 37 out of 43 cases recruited. Baseline PVL could be determined for 31 out of 43 cases recruited but could not be done at follow-up due to non-availability of kit and reagents. All cases in the study were started on HAART as per NACO guidelines. [1] Patients were asked to report to follow-up after a minimum period of three months to monitor the clinical and immunological response to HAART. On follow-up, the cases were categorised as clinical failure and immunological failure as per WHO guidelines. [4] CD4 cell count typically increases by> 50 cells/μL at four to eight weeks and an additional 50 to 100 cells/μL/year thereafter.[6] For quantitative data, difference between the mean was analysed by Wilcoxon sign rank test and unpaired data by Mann Whitney test while for qualitative data, proportions between the groups was compared by Chi-square test. Results All patients studied had a baseline CD4 cell count ranging from 7-195 cells/μL (mean 112 ± 60 cells/μL). CD4 cell count of < 50 cells/μL was seen in 18.6% patients signifying the stage of severe immunosuppression. Seventy two percent patients had a total lymphocyte count (TLC) ≤1200/mm 3 and 83% patients had CD4:CD8 ratio ≤0.2. The CD4 percentage was < 14 percent in 89.2% cases. The baseline plasma viral load (PVL) of 31 patients studied ranged from 1607-> 750000 copies/mL with a mean of 192,686 copies/mL. PVL was higher among patients with lower CD4 cell count as all patients with CD4 cell count ≤50 cells/μL had PVL> 100000 copies/mL. The most common presenting complaints in the patients studied were weight loss (74.4%), cough (72.1%) and diarrhoea (67.4%). Twenty one percent patients belonged to WHO clinical stage IV (mean CD4 cell count = 74.6 cells/μL), 51% to stage III (mean CD4 cell count = 103.9 cells/μL) and 28% to stage II (mean CD4 cell count = 155 cells/μL). Adherence to HAART was> 95% in the patients studied. Out of 43 patients, eight patients (19%) expired before reporting for follow-up and nine patients(21%) did not report for follow-up. Twenty six patients (60%) came for follow-up after a mean period of 4.7 months (range = 3 to 6 months). All patients who expired had a CD4 cell count between 7-69 cells/μL (mean 34.5 cells/μL) while PVL ranged from 1,67,739 -> 7,50,000 copies/mL (mean 4,24,548 copies/mL). Out of the 26 patients who came for follow-up, 21 patients (80.8%) showed clinical improvement, while clinical failure was suspected in five patients (19.2%) as seen in [Table - 1]. All patients who expired had a CD4 cell count between 7-69 cells/μL (mean 35.4 cell cells/μL) while PVL ranged from 1,67,739 - > 7,50,000 copies/mL(mean 4,24,548 copies/mL). Out of the 26 patients who came for follow-up, 21 patients (80.8%) showed cliniccal improvment, while clinical failure was suspected in five patients (19.2%) as seen in table 1. [Table - 2] shows the change in CD4 count after ≥3 months of HAART. All except four patients (15.4%) showed an increase of ≥50 CD4 cells/μL. Among these four cases, three also showed a clinical failure. In our study, mean CD4 cell count of patients who came for follow-up increased from 126 ± 16.6 cells/μL (median130 cells/μL) at baseline to 278 ± 196.7 cells/μL(median 238 cells/μL) (P < 0.001), mean total lymphocyte count (TLC) increased from 1621 ± 780.7/mm 3 (median 1200/mm 3 ) at baseline to 2491 ± 1242.4/mm 3 (median 2000/mm 3 ) ( P < 0.05). Among the patients who expired (8) and those who were alive at follow-up (26), a significant difference ( P < 0.001) was found between the baseline mean CD4 cell count (35 cells/μL vs 126 cells/μL), mean CD4% (3.7 vs 8.3), mean PVL (4,24,548 copies/mL vs 1,45,766 copies/mL) and mean TLC (700 mm 3 vs 1621 mm 3 ). Discussion As per NACO guidelines, currently in India, absolute CD4 cell count is being used as the basis for initiation of ART. [1] The validity of this approach in comparison to plasma viral load has not been studied widely in India. Baseline plasma viral load estimates are being carried out in very few patients because of limited resources. The present study was undertaken as a pilot study for this purpose. In the present study, baseline mean CD4 cell count was 112.1 ± 60.29 cells/μL and mean CD4:CD8 ratio was 0.14 ± 0.09 which is in agreement with studies among similar patient groups from other parts of India. [8],[9],[10] CDC has expanded the AIDS surveillance case definition to include all HIV-infected persons with CD4+ T-lymphocyte counts of less than 200 cells/μL or a CD4+ percentage of less than 14. [5] In our study, the CD4 percentage was < 14 in 89.2% cases with CD4 count < 200 cells/μL. In a study from the US, it is said that CD4 absolute count is the best predictor of an adverse event when the CD4 count is ≤200 cells/uL while CD4+ percentage is a better predictor when the CD4 count is ≥200 cells/µL. [11] In our study, at baseline, 70.3% patients had a total lymphocyte count (TLC) ≤1200/mm 3 which is in contrast with one study in Mozambique, in which the sensitivity of TLC to detect the cases with CD4 count < 200 cells/μL was only 48.9%.[12] However, a study from U.K showed that TLC is almost as reliable as CD4 count for prediction of AIDS defining opportunistic infections. [13] The threshold value for the dichotomisation of TLC was taken as 1200 cells/mm 3 , considered a marker of serious immunosuppression according to WHO for resource limited settings. [4] Eighty four pecent cases showed an increase of more than 50 cells/μL following HAART which is in concordance with another recent Indian study. [2] Our study showed a mean CD4 gain of 152 cells/μL within a mean duration of 4.7 months. However, another Indian study from Chennai has documented a mean CD4 gain of 188 cells/μL within a mean duration of 4.3 months. [3] A statistically significant increase in the mean TLC was also observed by us, which is in accordance with another study which showed that within the first two years of HAART, the direction of change in TLC appears to be concomitant with changes in CD4 count. [8] In conclusion, good treatment response to the HAART regimens being provided was observed in> 80% patients, implying that the HAART is efficacious and its efficacy would further increase if it will be given well in time, since initiation of therapy at an advanced stage of immunosuppression (≤50 cells/μL) may not be as effective. Those patients, who expired after the initiation of HAART, showed statistically significant lower baseline values of mean CD4 cell count, mean CD4+ percentage, mean total lymphocyte count and higher baseline value of mean HIV plasma viral load in comparison to the patients who were alive at follow-up. In places where CD4 count facilities are not available, total lymphocyte count ≤1200/mm 3 may be used as a surrogate marker of CD4 cell count < 200/μL, however, further studies are required in HIV patients with CD4 count 200-499/μL and ≥ 500/μL References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08079t2.jpg] [mb08079t1.jpg] |
| |||||||||
{kind=link}
{kind=link}