 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
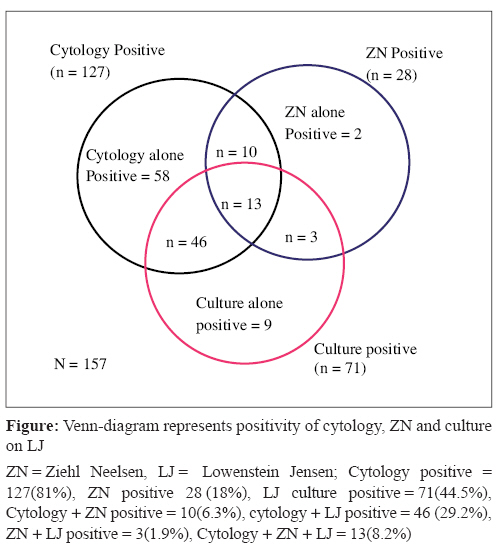
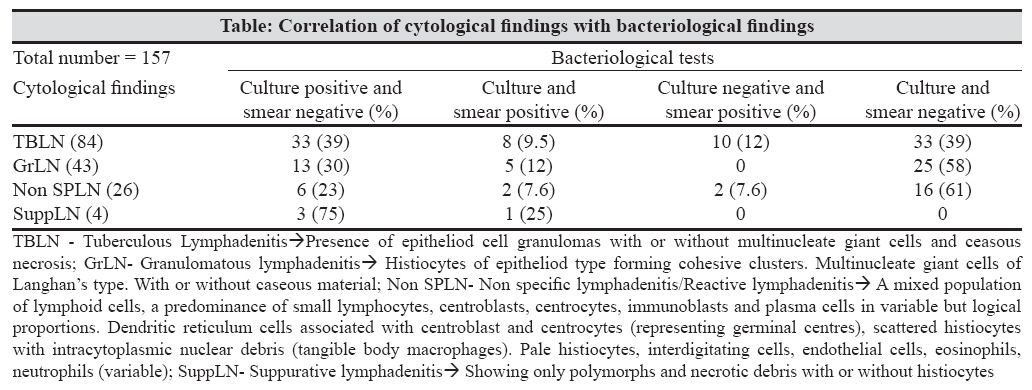
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 259-261 Brief Communication Mycobacterial culture of fine needle aspirate - A useful tool in diagnosing tuberculous lymphadenitis Kishore Reddy VC, Aparna S, Prasad CE, Srinivas A, Triveni B, Gokhale S, Krishna Moorthy KV Blue Peter Research Center-LEPRA Society, Hyderabad Date of Submission: 03-Aug-2007 Code Number: mb08080 Abstract A prospective study was undertaken on suspected lymph node TB (LNTB) patients, to evaluate the diagnostic utility of mycobacterial culture of fine needle aspirate (FNA), in comparison with the cytological examination and acid fast staining. Eighty percent of 157 aspirates studied were positive by cytological examination; 18% by ZN smear and 45% were positive by culture. Twelve aspirates which were negative by cytological features yielded positive mycobacterial cultures; four out of these were from HIV positive patients. Our observations suggest that supplementing FNA cytology with mycobacterial culture would increase the sensitivity of diagnosing LNTB; in addition to giving a highly specific diagnosis.Keywords: Extra pulmonary tuberculosis, fine needle aspiration, lymph node tuberculosis, culture Cervical lymphadenitis (LNTB) is the most common manifestation of extrapulmonary form of tuberculosis. LNTB has been increasingly observed in India with growing epidemic of HIV infection. [1] Standard diagnostic algorithm for LNTB in India, recommends fine needle aspiration cytology (FNAC) along with Ziehl-Neelsen staining (ZN) for acid fast bacilli in clinically suspected patients. [2] However, this has the disadvantage of non-specific findings on cytological examination and poor sensitivity by ZN smear. [3] Mycobacterial culture being a gold standard method could be useful as a tool for definitive diagnosis. [4] With this background, a prospective study was undertaken to determine the utility of mycobacterial culture of fine needle aspirate in addition to the cytology and ZN staining in diagnosis of LNTB. Materials and Methods Patients with clinically suspected LNTB, attending the clinics of LEPRA-Blue Peter Research Centre and AP State Chest hospital (Hyderabad) during 2004-05, were studied, after obtaining an informed consent. Information including detailed clinical examination, history of previous treatment with anti-tuberculous (anti-TB) drugs or broad spectrum antibiotics was recorded. All the patients were subjected for voluntary and confidential testing for HIV infection. The institutional ethical committee of Blue Peter Research Centre had approved the study protocol. Fine needle aspiration (FNA) was performed by either a pathologist or a clinician as described previously. [5] The aspirate was divided into three portions, one each for cytology, acid fast staining using 20% H 2 SO 4 and mycobacterial culture. Cytological examination by haematoxylin and eosin staining (H and E) and acid fast staining by Ziehl-Neelsen (Z N) method were carried out as described previously; [2],[5] smears were observed independently by pathologist and microbiologist respectively. Aspirate meant for mycobacterial culture was either inoculated immediately or preserved at 4 o C for not more than 24 hours before inoculation. All the aspirates were inoculated on two sterile Lowenstein-Jensen (LJ) medium slopes and incubated up to eight weeks at 37°C. Colonies grown on LJ were confirmed by ZN staining and biochemical tests as described previously. [6] Positive diagnosis of tuberculosis was considered when either of the following criteria was met; (i) presence of epithelioid cell granulomas with or without multinucleate giant cells and caseation necrosis on H and E staining (ii) demonstration of acid fast bacilli on Z N staining and/or (iii) isolation of mycobacteria on culture. [7] Results A total of 186 patients were enrolled in to the study; however, we have analysed the data of 157 patients, whose aspirates were adequate for conducting all the three tests. Twenty five patients (13.4%) out of 157 had a previous treatment with anti-TB drugs and 75% had treatment with broad spectrum antibiotics. HIV seropositivity was observed among 14.5 % patients. One or either of the laboratory tests was positive in 141/ 157 aspirates. Cytology was positive in 81% aspirates, 18% were ZN smear positive and 45% were positive by culture [Figure - 1]. Average duration taken for positive culture was 35 days (range 21-56 days). All the culture isolates were identified as Mycobacterium tuberculosis . The correlation between the cytological and bacteriological findings is shown in the table. Cytological diagnosis among aspirates from HIV seronegative patients showed 59% tuberculous lymphadenitis and 27% granulomatous lymphadenitis; where as it was 26%, and 30% respectively in HIV positive patients. Non-specific lymphadenitis was 14% and 30% among the respective two groups. However, suppurative lymphadenitis was observed (14.8%) only in HIV positive TB patients. Discussion Tuberculous lymphadenitis comprised about a half of 1,44,670 cases of extra pulmonary TB reported for the year 2005 in India. [8] This emphasises the need to study the diagnostic methods for LNTB. The present study explores the utility of FNA culture in diagnosing LNTB in a public health perspective. More than three quarters of the patients studied, were positively diagnosed by either one or more of the laboratory tests. Cytological examination of the fine needle aspirate seems to be the most sensitive test, however, including bacteriological tests may be more helpful, considering their ability to yield a definitive diagnosis. Revised national tuberculosis control program (RNTCP) in India recommends cytology and ZN smear of FNA for diagnosing LNTB. [8] This might have the disadvantages of low specificity due to cytological appearance sharing the similarities with other granulomatous conditions. In addition to this, aspirates tend to contain very small number of mycobacteria to be picked up by ZN smear alone. In this study, the sensitivity of the diagnosis was improved by supplementing cytology and ZN smear with culture [Figure - 1]. Despite the fact that mycobacterial culture facility is not widely available in India, attempts should always be made, wherever resources permit. About a half of the study aspirates that were positive by cytology were negative by culture [Table - 1]. We found that majority of culture negative aspirates were from patients who had a previous history of anti-TB treatment or prior usage of broad spectrum antibiotics for the lymph node swelling (data not shown). Existing guidelines recommend a three-week course of broad spectrum antibiotics before confirming the diagnosis in smear negative pulmonary as well as the lymph node TB. [2] Broad spectrum antibiotics such as amoxicillin - clavulanic acid and fluoroquinolones, have been reported to be inhibitory to M tuberculosis that might lead to negative initial sputum smears and cultures. [9] However, there is a paucity of literature on such findings in LNTB. We speculate that the cytology positive and culture negative results in the study could be due to the inhibitory effect of prior broad spectrum antibiotic or anti-TB treatment. There can also be a possibility for the presence of non viable or very few organisms that were missed by culture. [3],[10] Cytology on the other hand is an expression of immune response which may exist even in the absence of live organisms. This response does not always mean an active infection. Therefore, it is likely that the patients with positive cytological diagnosis but negative culture were in various stages of disease where viable mycobacteria might not exist in the lymph node. Though FNA cytology is presumed to be an established test for diagnosing LNTB, eight percent (12/157) of the aspirates which were positive by culture could not show the cytological features of tuberculosis. This suggests the need to add mycobacterial culture to cytology while diagnosing LNTB [Table - 1]. This is more so in HIV positive patients. We found that all the aspirates showing suppurative cellular response yielded positive mycobacterial culture (data not shown). Hence, it may be suggested that suppurative lymphadenitis in HIV positive individuals should make a high index of clinical suspicion for tuberculosis, in addition to warranting culture for a specific diagnosis. [1],[11] In conclusion, findings from the present study emphasise a definite need for a combination of tests for diagnosing LNTB. Though, it is not widely practiced, culture of FNA may be an additional and more specific tool. It is therefore suggested that bacteriological examination including mycobacterial culture may be considered for diagnosing LNTB wherever it is possible. FNA culture facility should be made available at least in a few referral centers to help in more accurate diagnosis in problem cases. Acknowledgement We thank the medical Officers and staff of Blue peter research centre and AP chest hospital for providing the patient data.References
Copyright 2008 - Indian Journal of Medical Microbiology Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 259-261 Brief Communication Mycobacterial culture of fine needle aspirate - A useful tool in diagnosing tuberculous lymphadenitis Kishore Reddy VC, Aparna S, Prasad CE, Srinivas A, Triveni B, Gokhale S, Krishna Moorthy KV Blue Peter Research Center-LEPRA Society, Hyderabad Date of Submission: 03-Aug-2007 Code Number: mb08080 Abstract A prospective study was undertaken on suspected lymph node TB (LNTB) patients, to evaluate the diagnostic utility of mycobacterial culture of fine needle aspirate (FNA), in comparison with the cytological examination and acid fast staining. Eighty percent of 157 aspirates studied were positive by cytological examination; 18% by ZN smear and 45% were positive by culture. Twelve aspirates which were negative by cytological features yielded positive mycobacterial cultures; four out of these were from HIV positive patients. Our observations suggest that supplementing FNA cytology with mycobacterial culture would increase the sensitivity of diagnosing LNTB; in addition to giving a highly specific diagnosis.Keywords: Extra pulmonary tuberculosis, fine needle aspiration, lymph node tuberculosis, culture Cervical lymphadenitis (LNTB) is the most common manifestation of extrapulmonary form of tuberculosis. LNTB has been increasingly observed in India with growing epidemic of HIV infection. [1] Standard diagnostic algorithm for LNTB in India, recommends fine needle aspiration cytology (FNAC) along with Ziehl-Neelsen staining (ZN) for acid fast bacilli in clinically suspected patients. [2] However, this has the disadvantage of non-specific findings on cytological examination and poor sensitivity by ZN smear. [3] Mycobacterial culture being a gold standard method could be useful as a tool for definitive diagnosis. [4] With this background, a prospective study was undertaken to determine the utility of mycobacterial culture of fine needle aspirate in addition to the cytology and ZN staining in diagnosis of LNTB. Materials and Methods Patients with clinically suspected LNTB, attending the clinics of LEPRA-Blue Peter Research Centre and AP State Chest hospital (Hyderabad) during 2004-05, were studied, after obtaining an informed consent. Information including detailed clinical examination, history of previous treatment with anti-tuberculous (anti-TB) drugs or broad spectrum antibiotics was recorded. All the patients were subjected for voluntary and confidential testing for HIV infection. The institutional ethical committee of Blue Peter Research Centre had approved the study protocol. Fine needle aspiration (FNA) was performed by either a pathologist or a clinician as described previously. [5] The aspirate was divided into three portions, one each for cytology, acid fast staining using 20% H 2 SO 4 and mycobacterial culture. Cytological examination by haematoxylin and eosin staining (H and E) and acid fast staining by Ziehl-Neelsen (Z N) method were carried out as described previously; [2],[5] smears were observed independently by pathologist and microbiologist respectively. Aspirate meant for mycobacterial culture was either inoculated immediately or preserved at 4 o C for not more than 24 hours before inoculation. All the aspirates were inoculated on two sterile Lowenstein-Jensen (LJ) medium slopes and incubated up to eight weeks at 37°C. Colonies grown on LJ were confirmed by ZN staining and biochemical tests as described previously. [6] Positive diagnosis of tuberculosis was considered when either of the following criteria was met; (i) presence of epithelioid cell granulomas with or without multinucleate giant cells and caseation necrosis on H and E staining (ii) demonstration of acid fast bacilli on Z N staining and/or (iii) isolation of mycobacteria on culture. [7] Results A total of 186 patients were enrolled in to the study; however, we have analysed the data of 157 patients, whose aspirates were adequate for conducting all the three tests. Twenty five patients (13.4%) out of 157 had a previous treatment with anti-TB drugs and 75% had treatment with broad spectrum antibiotics. HIV seropositivity was observed among 14.5 % patients. One or either of the laboratory tests was positive in 141/ 157 aspirates. Cytology was positive in 81% aspirates, 18% were ZN smear positive and 45% were positive by culture [Figure - 1]. Average duration taken for positive culture was 35 days (range 21-56 days). All the culture isolates were identified as Mycobacterium tuberculosis . The correlation between the cytological and bacteriological findings is shown in the table. Cytological diagnosis among aspirates from HIV seronegative patients showed 59% tuberculous lymphadenitis and 27% granulomatous lymphadenitis; where as it was 26%, and 30% respectively in HIV positive patients. Non-specific lymphadenitis was 14% and 30% among the respective two groups. However, suppurative lymphadenitis was observed (14.8%) only in HIV positive TB patients. Discussion Tuberculous lymphadenitis comprised about a half of 1,44,670 cases of extra pulmonary TB reported for the year 2005 in India. [8] This emphasises the need to study the diagnostic methods for LNTB. The present study explores the utility of FNA culture in diagnosing LNTB in a public health perspective. More than three quarters of the patients studied, were positively diagnosed by either one or more of the laboratory tests. Cytological examination of the fine needle aspirate seems to be the most sensitive test, however, including bacteriological tests may be more helpful, considering their ability to yield a definitive diagnosis. Revised national tuberculosis control program (RNTCP) in India recommends cytology and ZN smear of FNA for diagnosing LNTB. [8] This might have the disadvantages of low specificity due to cytological appearance sharing the similarities with other granulomatous conditions. In addition to this, aspirates tend to contain very small number of mycobacteria to be picked up by ZN smear alone. In this study, the sensitivity of the diagnosis was improved by supplementing cytology and ZN smear with culture [Figure - 1]. Despite the fact that mycobacterial culture facility is not widely available in India, attempts should always be made, wherever resources permit. About a half of the study aspirates that were positive by cytology were negative by culture [Table - 1]. We found that majority of culture negative aspirates were from patients who had a previous history of anti-TB treatment or prior usage of broad spectrum antibiotics for the lymph node swelling (data not shown). Existing guidelines recommend a three-week course of broad spectrum antibiotics before confirming the diagnosis in smear negative pulmonary as well as the lymph node TB. [2] Broad spectrum antibiotics such as amoxicillin - clavulanic acid and fluoroquinolones, have been reported to be inhibitory to M tuberculosis that might lead to negative initial sputum smears and cultures. [9] However, there is a paucity of literature on such findings in LNTB. We speculate that the cytology positive and culture negative results in the study could be due to the inhibitory effect of prior broad spectrum antibiotic or anti-TB treatment. There can also be a possibility for the presence of non viable or very few organisms that were missed by culture. [3],[10] Cytology on the other hand is an expression of immune response which may exist even in the absence of live organisms. This response does not always mean an active infection. Therefore, it is likely that the patients with positive cytological diagnosis but negative culture were in various stages of disease where viable mycobacteria might not exist in the lymph node. Though FNA cytology is presumed to be an established test for diagnosing LNTB, eight percent (12/157) of the aspirates which were positive by culture could not show the cytological features of tuberculosis. This suggests the need to add mycobacterial culture to cytology while diagnosing LNTB [Table - 1]. This is more so in HIV positive patients. We found that all the aspirates showing suppurative cellular response yielded positive mycobacterial culture (data not shown). Hence, it may be suggested that suppurative lymphadenitis in HIV positive individuals should make a high index of clinical suspicion for tuberculosis, in addition to warranting culture for a specific diagnosis. [1],[11] In conclusion, findings from the present study emphasise a definite need for a combination of tests for diagnosing LNTB. Though, it is not widely practiced, culture of FNA may be an additional and more specific tool. It is therefore suggested that bacteriological examination including mycobacterial culture may be considered for diagnosing LNTB wherever it is possible. FNA culture facility should be made available at least in a few referral centers to help in more accurate diagnosis in problem cases. Acknowledgement We thank the medical Officers and staff of Blue peter research centre and AP chest hospital for providing the patient data.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08080f1.jpg] [mb08080t1.jpg] |
| |||||||||
{kind=link}
{kind=link}