 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
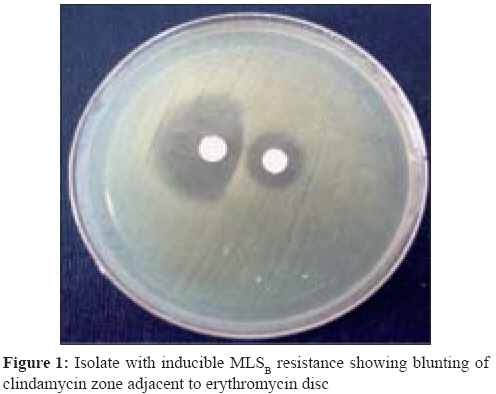
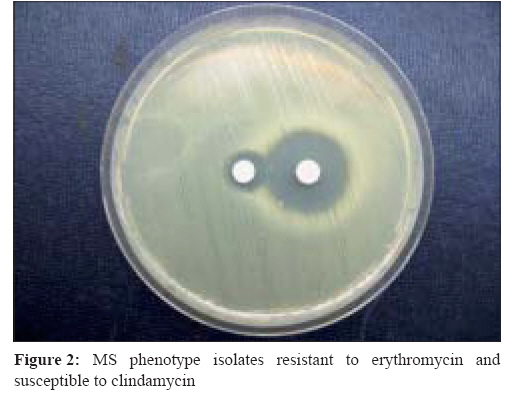
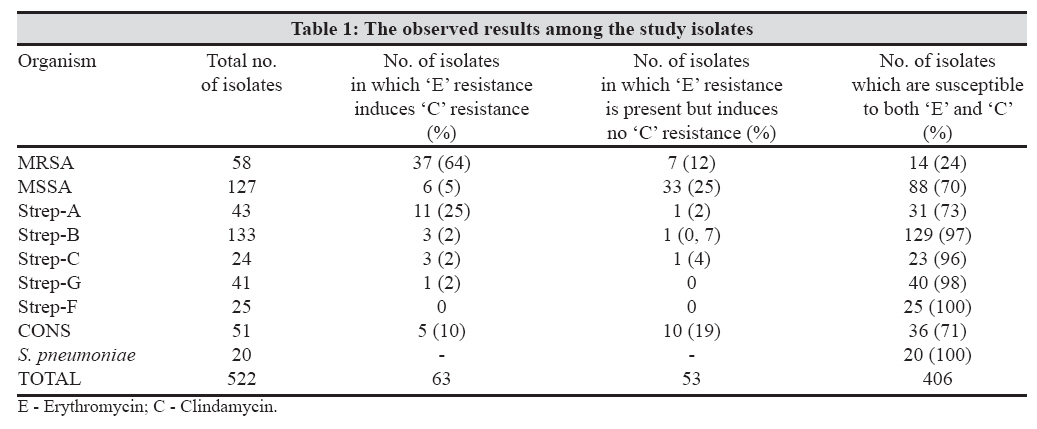
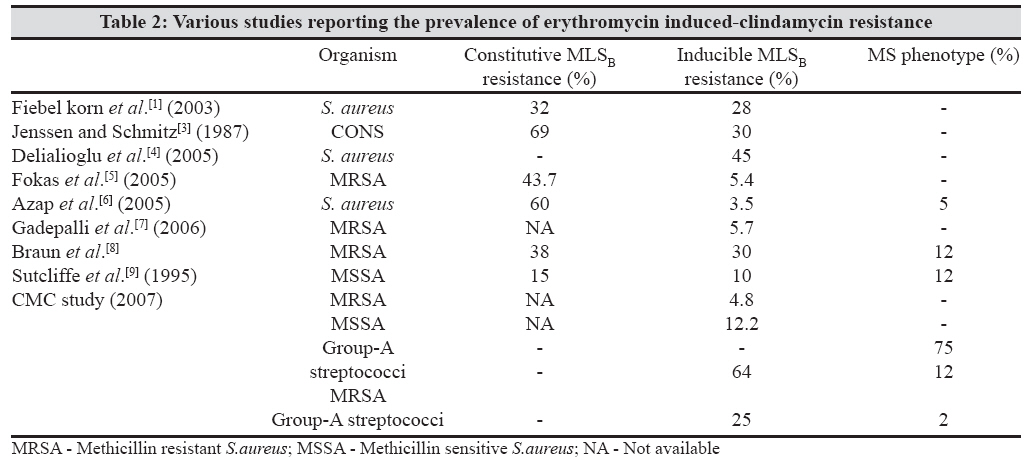
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 262-264 Brief Communication Prevalence of inducible clindamycin resistance in gram positive organisms in a tertiary care centre Angel MR, Balaji V, Prakash JAJ, Brahmadathan KN, Mathews MS Department of Clinical Microbiology, Christian Medical College and Hospital, Vellore - 632 004 Date of Submission: 19-Sep-2007 Code Number: mb08081 Abstract Gram positive organisms are one of the leading pathogens causing skin and soft tissue infections. For these infections, clindamycin is a useful alternate drug in penicillin-allergic patients. This study was conducted to investigate the prevalence of erythromycin-induced clindamycin resistance in gram positive organisms in the southern part of the country. A total of 522 consecutive clinical isolates from blood, CSF, sputum, throat, pus, and urine were collected between November 2006 and April 2007 and tested for erythromycin resistance and inducible clindamycin resistance. There was a relatively higher incidence of inducible clindamycin resistance among the MRSA isolates. We conclude, therefore, that clindamycin is not a suitable alternative antibiotic for use in staphylococcal skin and soft tissue infections.Keywords: Clindamycin, erythromycin, gram-positive organisms Clindamycin is considered an useful alternate drug in penicillin-allergic patients in the treatment of skin and soft tissue infections caused by Staphylococcus aureus . It has excellent tissue penetration (except for the central nervous system), accumulates in abscesses, and no dosage adjustments are required in the presence of renal disease. [1] The good oral absorption of clindamycin makes it an attractive option for use in outpatients or as follow-up treatment after intravenous therapy (de-escalation). Staphylococcus spp. can be resistant to erythromycin through either erm or msr A genes. Strains with erm -mediated erythromycin resistance may possess inducible clindamycin resistance but may appear susceptible to clindamycin by disc diffusion. [1] If inducible resistance can be reliably detected on a routine basis in clinically significant isolates, clindamycin can be safely and effectively used only in those patients with truly clindamycin-susceptible strains. We investigated the prevalence of erythromycin-induced clindamycin resistance in gram-positive organisms as there were no data available from the southern part of the country. Materials and Methods A total of 522 consecutive clinical isolates from blood, CSF, sputum, throat, pus, and urine were collected between November 2006 and April 2007 and tested for erythromycin resistance and inducible clindamycin resistance. These isolates included methicillin-resistant S. aureus ( n = 58), methicillin-susceptible S. aureus ( n = 127), coagulase-negative Staphylococcus ( n = 51), group A Streptococcus ( n = 43), group B Streptococcus ( n = 133), group C Streptococcus ( n = 24), group G Streptococcus ( n = 41), group F Streptococcus ( n = 25), and Streptococcus pneumoniae ( n = 20). Double-disk diffusion test was carried out as per CLSI guidelines. [2] Briefly, the disk approximation test was performed with erythromycin (15 μg) and clindamycin (2 μg) 15 mm apart on the same plate [Figure - 1],[Figure - 2]. S. aureus American Type Culture Collection (ATCC) BAA-977 (containing inducible erm A-mediated resistance; inducible MLS B resistance) and S. aureus ATCC BAA-976 (containing inducible msr A-efflux mediated macrolide resistance; MS phenotype) were used as quality control isolates. S. aureus ATCC BAA-977 showed inducible clindamycin resistance (i.e., a positive D-zone test), while S. aureus ATCC BAA-976 showed noninducible clindamycin resistance. S. aureus ATCC 25923 was used for routine quality control of erythromycin and clindamycin disks using Mueller-Hinton agar. [1] Results The observed results among these study isolates are depicted in [Table - 1]. This study revealed a relatively higher incidence of inducible clindamycin resistance among the methicillin resistant S. aureus (MRSA) isolates.Discussion Various studies reporting the prevalence of erythromycin-induced clindamycin resistance is shown in [Table - 2]. Interestingly, there has been no constitutive MLS B resistance observed to date among S. aureus clinical isolates recovered from this centre. This was in agreement with the finding of Jenssen et al. [3] ; however, the majority of other studies reported constitutive MLS B resistance, [1],[4],[5] including Gadepalli et al [7] from North India. Among the β-haemolytic streptococcal isolates, there was no constitutive MLS B resistance, which is similar to another study. [9] Also in agreement with another study, [10] our S. pneumoniae study isolates did not have constitutive resistance. In conclusion, we found that clindamycin is not a suitable alternative drug in staphylococcal infections because of the high level of inducible clindamycin resistance among the MRSA isolates. In addition, the MS phenotype found in India appears to differ from those in other countries References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08081t1.jpg] [mb08081f2.jpg] [mb08081f1.jpg] [mb08081t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}