 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
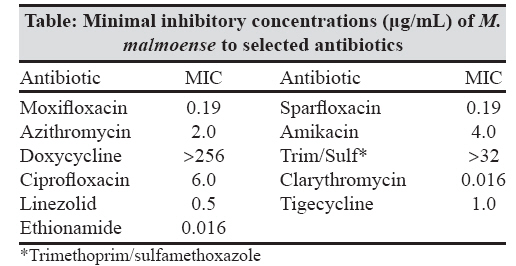
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 267-269 Case Report Isolation of Mycobacterium malmoense in the island of Crete, Greece Kourbeti IS, Neonakis IK, Gitti Z, Spandidos DA Department of Internal Medicine University Hospital of Heraklion, 71201 Heraklion Date of Submission: 01-Oct-2007 Code Number: mb08083 Abstract Mycobacterium malmoense was isolated from a broncho-alveolar lavage sample of a 73-year-old cancer (small cell lung carcinoma) patient in Crete, representing the first reported case of this pathogen in Greece. The isolate was considered to be a colonizer and the patient did not receive any antimycobacterial treatment while he received chemotherapy to which he responded favourably. No signs of pulmonary infection were noted during the course of his disease. This case provides evidence of the ubiquitous nature of this mycobacterial species, believed until recently to favour cooler climates. We, therefore, propose that the index of suspicion for this pathogen should be raised particularly in patients with underlying immunodeficiency, cancer and chronic lung disease, irrespective of the geographic location.Keywords: Greece, Mycobacterium malmoense, nontuberculous mycobacteria Over the last few years, there is an increasing appreciation for the role of nontuberculous mycobacteria (NTM) as pathogens especially in immunocompromised patients. [1] The introduction of molecular techniques has facilitated the detection and identification of new NTM species, the role of which is under constant evaluation. [2] Mycobacterium malmoense is a slowly growing NTM that has attracted global interest due to its increased pathogenicity. [3] It is most frequently isolated in cool climates such as Northern and Central Europe. We report on the first isolation of the pathogen from a clinical specimen in the island of Crete, and we describe the drug susceptibility profile of the isolate. Case Report A 73-year-old male with past medical history of smoking (86 pack-years) and diabetes mellitus Presented in October 2006 complaining of abdominal pain, nausea, vomiting and a weight loss of 6 kg. The physical examination revealed right upper quadrant tenderness and an enlarged liver. The baseline laboratory investigation showed a marked increase in the γGT (16-fold), and LDH (7-fold). The chest radiography was consistent with an increase in size of the right hilum. Bronchoscopy revealed a submucosal infiltration of the right bronchial tree. The chest computed tomography (CT) showed a mass of 10 cm x 8 cm. There were small pulmonary satellite nodular lesions and enlarged paratracheal and subcarinal lymph nodes. The lung biopsy revealed small cell lung cancer (SLCC). Abdominal CT revealed multiple liver metastases. A broncho-alveolar lavage (BAL) sample was sent for mycobacterial culture among other laboratory examinations. Acid-fast staining of the BAL sample was negative. The liquid culture (BacT/Alert 3D; bioMιrieux, Durham, NC) turned positive after 35.6 days, followed by a positive solid culture (Lowenstein-Jensen; bioMιrieux, Marcy l′ Etoile, France) four days later. The AccuProbe assay for Mycobacterium tuberculosis complex (Gen-Probe, San Diego, CA) was negative, indicative of the presence of an NTM. GenoType Common Mycobacteria (GenoType CM) and GenoType Additional Species assay (GenoType AS, Hain Lifescience, Nehren, Germany) were subsequently performed, establishing the diagnosis of M. malmoense by molecular hybridization. Drug susceptibilities were determined by the conventional proportions method. The strain was resistant to isoniazid (1μg/mL; INH), ethambutol (3μg/mL; EMB) and para-4-aminosalicylic acid (0.5μg/mL; PAS). It was sensitive to rifampicin (20μg/mL; RIF), pyrazinamide (200μg/mL; PZA) and streptomycin (4μg/mL; SM). The minimal inhibitory concentrations (MICs) of the strain to a panel of additional antibiotics were determined by means of the E test methodology (AB Biodisk, Solna, Sweden). The results [Table - 1] showed that the isolate was resistant to doxycyline, and trimethoprim/sulfamethoxazole, whereas it was susceptible to clarithromycin and ethionamide. The less active molecules were ethambutol, amikacin and ciprofloxacin. The isolate was considered to be a coloniser and the patient did not receive any antimycobacterial treatment while he received chemotherapy for SCLC. He responded favourably to the chemotherapy. No signs of pulmonary infection were noted during the course of his disease. Discussion Mycobacterium malmoense was first described in 1977 in the Swedish city of Malmo. [4] It is a non-pigmented, slow growing mycobacterium that grows best at 30°C and at a low pH (between 5.0 and 6.0). It has been isolated from the environment only on very rare occasions. [5] The discrimination between genuine disease and mere contamination can be very difficult. M. malmoense is considered among the NTM that carry an increased pathogenicity, especially in patients with underlying disease such as immunodeficiency, cancer or chronic lung disease. [3] Its clinical relevance has been shown to be extraordinarily high (67%), much more than the rate of most frequently encountered NTM. [6] According to another study, 92% of a series of patients from whom M. malmoense was cultured even as a single isolation had evidence of active pulmonary disease, something that has also been validated by more recent reports. [3],[7] Despite the fact that in the United States there was an increasing number of isolates, the number of patients with confirmed M. malmoense infection remains low. [8] The organism has been isolated mainly from respiratory specimens but also from lymph nodes (especially in children where the disease presents as lymphadenitis), stools, cutaneous, tendon and synovial biopsies [8] and abscess pus. [3] The patient we report in this study suffered from SCLC with no symptoms suggestive of an NTM infection. Among the CT findings, the reported nodules were suspicious although they were satellite to the malignant mass and they were considered to be malignant, as well as the enlarged mediastinal lymph nodes. M. malmoense clinical isolates are mainly reported from Northern and Central Europe (United Kingdom, Sweden, Finland, Switzerland, Belgium, France and Austria) and Northern America [8],[9] with only a few cases from southern Europe. [6] For this reason, M. malmoense has generally been thought to be a pathogen restricted to cooler climates, thus there was a limited awareness of this organism in southern European countries such as Italy or Greece. [6] As a result, no efforts have been made to use more appropriate cultural procedures for M. malmoense isolation, such as lower incubation temperatures and the use of acid media. Its isolation in Crete suggests that M. malmoense is a ubiquitous organism and the initial recognition of its role as a pathogen in cooler regions might have only been coincidental. Our isolate was found to be sensitive to RIF, PZA and SM but resistant to INH and EMB. Significant differences in the susceptibility patterns may occur among isolates, but in vitro resistance to antimycobacterial drugs does not necessarily predict failure of treatment or relapse. [10] Synergism among drugs could be an explanation. [10] In conclusion, we report the first isolation of M malmoense from a clinical specimen in Greece. This should increase the awareness for the ubiquity of this species and raise the index of suspicion for the detection of the pathogen, particularly, in immunocompromised patients. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08083t1.jpg] |
| |||||||||
{kind=link}