 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
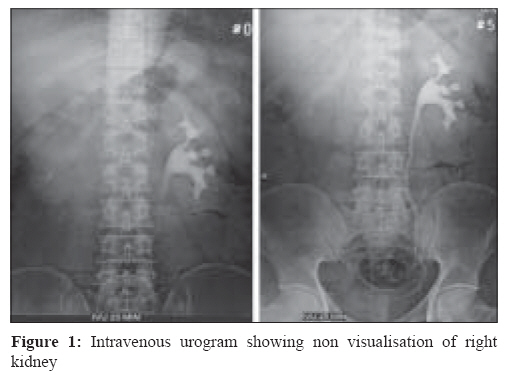
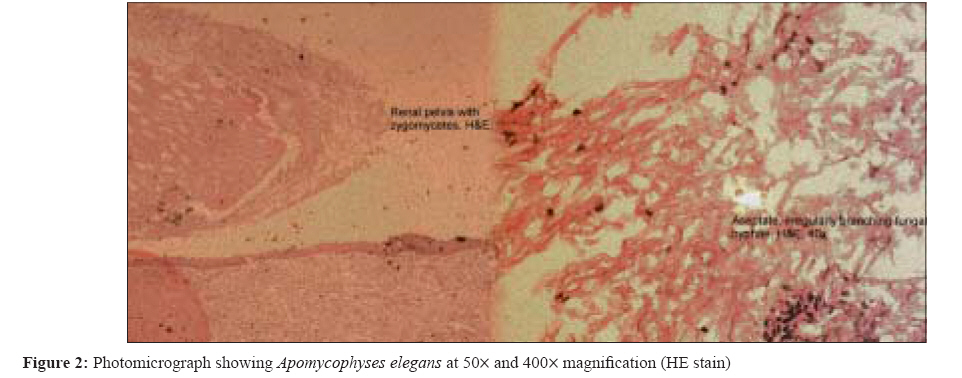
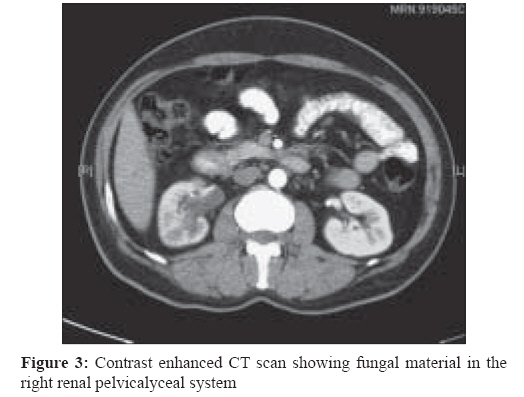
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 269-271 Case Report Apophysomyces elegans - renal mucormycosis in a healthy host: A case report from south India Thomas AJ, Shah S, Mathews MS, Chacko N Department of Urology, Christian Medical College, Vellore - 632 004, Tamil Nadu Date of Submission: 25-Jan-2008 Code Number: mb08084 Abstract Zygomycosis is an opportunistic fungal infection that seldom occurs in individuals with a competent immune system. Isolated involvement of any organ is rare and only a few cases of renal zygomycosis have been reported. We present an unusual case of renal zygomycosis caused by Apophysomyces elegans in a patient with no known predisposing factor. He presented with flakes in the urine and was found to have a poorly functioning right kidney. Ureterorenoscopy was performed, fungal elements removed and pathological confirmation obtained. The patient subsequently underwent nephrectomy after treatment with amphotericin B. He made an uneventful recovery.Keywords: Apomycophyses elegans, renal mucormycosis Zygomycosis (mucormycosis) is caused by fungi of the order Mucorales and most commonly by organisms belonging to genus Rhizopus . Others include Absidia, Mucor, Apophyomyces and Saksenaea . [1],[2] Renal involvement in disseminated mucormycosis occurs in up to 19% of patients. [3] Isolated renal zygomycosis (mucormycosis) is extremely rare. Only few cases caused by varied species have been reported. [1],[4],[5],[6],[7],[8],[9] To the best of our knowledge, this is the first report of renal zygomycosis (mucormycosis) caused by Apophysomyces elegans from the south of the country, in a patient who was otherwise healthy. Case Report A 41-year-old male presented on 2 nd March 2006 to the urology out patient department at the authors′ institution with passage of whitish flakes in the urine for three months. He had occasional burning micturition and a vague ache in the right flank, neither of which was bothersome. There was no fever, haematuria, calculuria, and loss of appetite or weight. He was not a diabetic but was recently detected to be hypertensive. He denied any history of surgical intervention or instrumentation. Physical examination was normal. A preoperative intravenous urogram revealed faint opacification of the right pelvicalyceal system with mild hydronephrosis [Figure - 1]. The right ureter was not visualised. The left side was normal. Urinary tests for acid fast bacilli (AFB) were negative. On cystoscopy, the urethra, ureteric orifices and bladder were normal. A retrograde pyelogram revealed a dilated ureter with filling defects in the ureter and pelvicalyceal system. Ureterorenoscopy disclosed fluffy dirty grey material in the ureter and pelvicalyceal system. Some of this was removed through the ureterorenoscope and sent for culture and histopathology examination. Direct microscopy of the material revealed aseptate fungal hyphae morphologically suggestive of zygomycetes. On culture of the material the organism was identified as Apophysomyces elegans [Figure - 2]. A preoperative CT revealed residual fungal material in the right pelvicalyceal system [Figure - 3]. He was subsequently treated with amphotericin B and underwent right nephrectomy. His recovery was uneventful and is asymptomatic after 6 months of follow up. His urine culture showed no growth Discussion Zygomycosis in humans is rare and the condition even rarer when patient is healthy with absent predisposing factors. [3],[10] To our knowledge, this is the first case to be reported from South India where a healthy individual presented with an isolated renal zygomycosis. The largest series of zygomycoses had 129 patients of which 11 had isolated involvement of kidneys. Apophysomyces elegans was isolated in only one patient. It is unclear whether this patient was asymptomatic. [3] Working differential diagnoses of renal TB and fungal bezoars were considered before proceeding to obtain a definitive diagnosis on histology and microbiological studies. Once the tissue confirmation was received a literature search was made on the mode of management. It is widely agreed that an aggressive approach needs to be pursued in order to care for what is believed to be a condition with a high mortality. [10] Treatment with anti-fungals preferably amphotericin B, followed with early nephrectomy is probably the best approach. [3] The patient received amphotericin B (0.6 mg/kg/day) and a nephrectomy was performed two days later. The antifungal treatment was continued for five days post operatively. Most reports are cases with a predisposing factor leading to a compromised immune status like diabetes, AIDS, drug abuse, and transplant recipients. [4],[5],[6],[7],[8],[9] It is not known whether they can present with minimal constitutional symptoms in a healthy individual. Also not known is whether a course of amphotericin B after the endoscopic removal of the fungal bezoars would have sufficed in an otherwise healthy patient like this. Since the fungus has a propensity to invade the blood vessels and cause infarction, drug penetration into the affected tissue remains inadequate - hence the need for a nephrectomy. [6] Rogenes et al , did a literature search of all such case reports and concluded that none of the cases that underwent a conservative line of management survived, in spite of receiving amphotericin B. [10] Only one patient who did not receive the drug is known to have survived. [10] Overall survival for isolated renal zygomycosis is estimated to be 65%. [10]. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08084f3.jpg] [mb08084f2.jpg] [mb08084f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}