 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
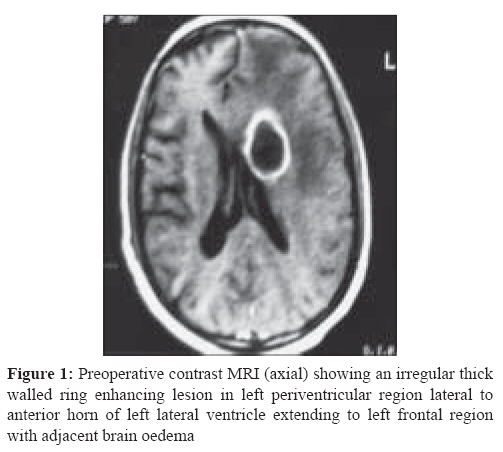
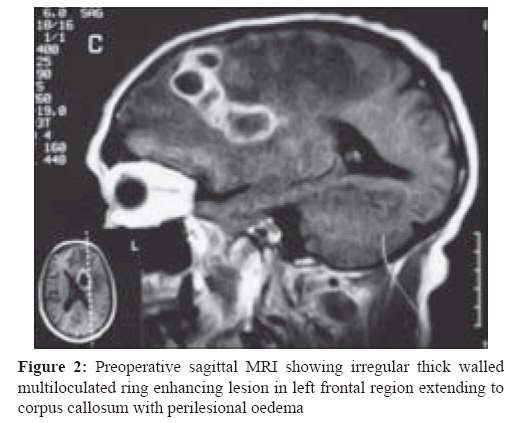
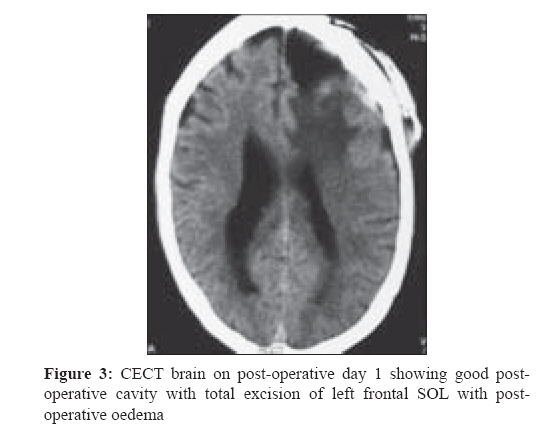
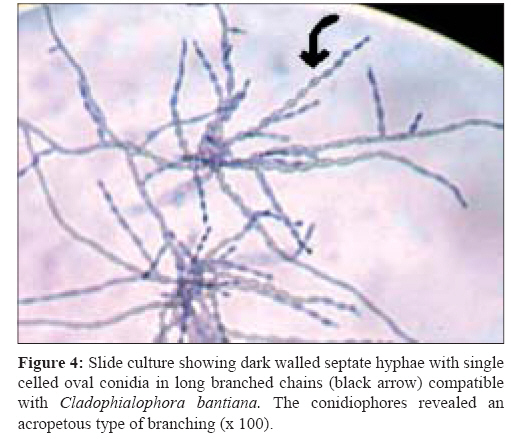
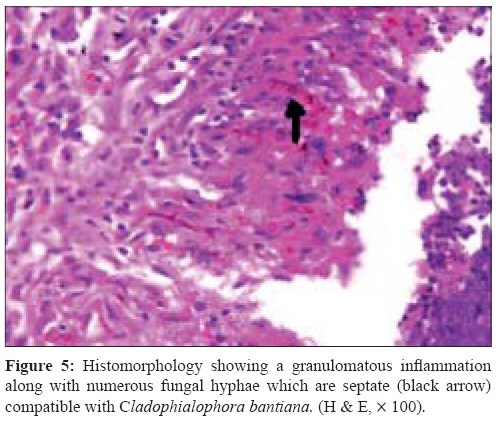
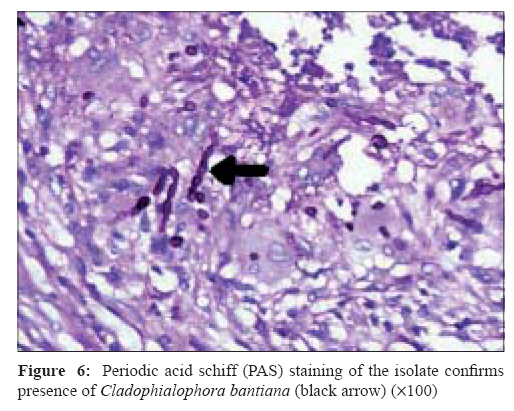
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 271-274 Case Report Brain abscess caused by Cladophialophora Bantiana in an immunocompetent host: Need for a novel cost-effective antifungal agent Borkar SA, Sharma MS, Rajpal G, Jain M, Xess I, Sharma BS Department of Neurosurgery, All India Institute of Medical Sciences, New Delhi-110 029 Date of Submission: 02-Jan-2008 Code Number: mb08085 Abstract We report a 53-year-old male who presented with headache, tremor and memory disturbance. Radiological evaluation was suggestive of brain abscess. He underwent gross total excision of the cerebral abscess. The histopathological examination and pus culture was suggestive of brain abscess caused by Cladophialophora bantiana. Authors report a rare case of biopsy and culture proven Cladophialophora bantiana brain abscess in an immunocompetent host. The authors review the relevant literature and current treatment options while emphasizing the need for a cost-effective novel antifungal drug to salvage a subset of patients suffering from this rare but increasingly frequent condition. Keywords: Brain abscess, Cladophialophora bantiana, central nervous system fungal infections, immunocompetence, management, surgery Phaeohyphomycosis is a term used to describe infections caused by dematiaceous fungi, i.e., fungi which contain melanin in their cell wall. [1] Cladophialophora bantiana has been implicated to cause brain abscess in immunocompromised patients including solid-organ transplant recipients and those with congenital or acquired immunodeficiency. [2],[3],[4],[5],[6] Brain abscess caused by Cladophialophora bantiana in an immunocompetent host is relatively rare. We report a case of brain abscess caused Cladophialophora bantiana in an immunocompetent host without any predisposing factor. Case Report A 55-year-old male presented to our outpatient clinic on 15 th March 2007 with complaints of bifrontal headache, personality change and increasing forgetfulness for the last three months. His relatives had also noticed altered behaviour and increasing forgetfulness since three months. He did not give any history of preceding trauma, vomiting, seizures, loss of consciousness, fever, sensorimotor or bladder-bowel disturbances. There was no significant past history of immunosuppresion, tuberculosis or diabetes mellitus. General examination of the patient did not reveal any abnormality except for slightly unsteady gait. He was afebrile, alert, well oriented. Visual acuity - right eye 6/6, left eye 6/9, on fundus examination there was no evidence of papilloedema. There were no sensorimotor and cranial nerve deficits. There were no cerebellar signs. Preoperative Gadolinium enhanced magnetic resonance imaging (MRI) scan showed an irregular thick walled ring enhancing lesion in left periventricular region extending to left frontal region [Figure - 1],[Figure - 2]. A provisional diagnosis of left frontal tuberculoma was made and the patient was started on anti tubercular drugs along with anticonvulsant (phenytoin), decongestant (glycerol) and steroids (dexamethasone) and posted for surgery. Preoperative haematological and biochemical parameters were normal. Left frontoparietal quadrangular flap craniotomy with gross total excision of left frontal space occupying lesion (SOL) was performed. Intraoperatively, there was a well defined multiloculated purulent collection bound by thick moderately vascular wall with adhesion to left lateral ventricle with intraventricular flakes in left frontal region. Postoperative contrast-enhanced computerised tomography (CECT) brain showed good postoperative cavity with total excision of SOL with no peripheral enhancement with mild oedema [Figure - 3]. Direct Gram stained preparation of pus revealed pus cells, but no bacteria. The smear stained by Ziehl Neelsen method (20% H 2 SO 4 ) was also negative for acid fast bacilli. Pus for bacterial culture and sensitivity was sterile. Potassium hydroxide (KOH) preparation of smear showed numerous septate hyphae. Frozen section of the specimen showed fungal hyphae with inflammatory granulation. Sample was further cultured on Sabouroud dextrose agar (SDA) plain, SDA with gentamicin, SDA with actidione. The tubes were incubated at 35°C and 25°C. After 72 hours of incubation, the tube showed colonies with an olive gray velvety appearance with a black undersurface. For identification, slide culture was done which showed dark walled septate hyphae with single celled oval conidia in long branched chains [Figure - 4]. Hyphae were septate and darkly pigmented with many conidia attached to the sides and lying free. Conidia were one-celled, pale brown, smooth-walled, and ellipsoid in shape. The conidiophores showed an acropetous type of braching [Figure - 4]. The isolate could be grown at 42°C and was also urease positive, features which differentiate C. bantiana from other morphologically similar saprophytic fungi. Histopathological examination also showed a granulomatous inflammation along with numerous septate fungal hyphae compatible with Cladosporium [Figure - 5]. The fungal profiles was confirmed by special stains (PAS, [Figure - 6]). There was no apparent source of fungus in his body. His tracheal, urine, blood cultures for fungus were negative. CSF staining and culture for fungus was also negative. CSF examination showed leucocytosis and increase in protein. Chest x-ray and CECT chest were normal. Patient was thoroughly investigated for any evidence of immunosuppresion. His HIV status was negative with normal CD4 count. Fasting and post prandial blood sugar were normal. He was not receiving any immnuosuppresive medication. Patient was put on intravenous amphotericin B and fluconazole 200 mg twice daily. Patient could not afford voriconazole and therefore it was not given. Patient had subjective improvement in tremors and headache and was well at the time of discharge with the advice to take anti fungal medications - intravenous amphotericin B total cumulative dose 3 gm with fluconazole 200 mg twice daily. Patient had a progressively downhill course in the follow-up period. MRI done at sixth month follow-up visit showed development of multiple brain abscesses. Patient was put on liposomal amphotericin B along with fluconazole, but the patient could not survive and died after four months. Discussion Phaeohyphomycosis is a term used to describe infections caused by fungi that contain melanin in their cell walls. [1] Cladophialophora bantiana is a soil-based neurotropic fungus, which has been implicated as a leading cause of cerebral phaeohyphomycosis because of its affinity to glial tissue. Pathogenicity is due to melanin which can scavange free radicals produced by phagocytic cells. In a recent case series published by Revankar et al , it accounted for 48 cases of CNS phaeohyphomycosis out of 101 cases reviewed. [1] Although the portal of entry is not clearly established, most probably it is through respiratory tract. Inhalation of spores followed by haematogenous dissemination to brain is the likely possibility. [1] Other sources can be from paranasal sinus (allergic fungal sinusitis) or direct inoculation in brain. In our patient, source of fungus was most probably from soil as he was involved in farming as his side business. In previously published reports, Cladophialophora brain abscess was common especially in immunocompromised patients and those receiving organ transplant, [2],[3],[4],[5],[6] but as per the recent series, it is on the rise even in immunocompetent hosts. [1] Percentage of immunosuppression varied from 23-50% and survival rate varied from 34-73%. This condition is highly fatal and mortality rates are almost equal among immunocompromised and immunocompetent patients. [1] CSF culture for fungus is positive less often and to the best of our knowledge only three culture positive cases of Cladophialophora bantiana meningitis have been reported till date. [7],[8],[9] Headache followed by focal neurological deficit are the most common presentation of Cladophialophora brain abscess. [1] Most important determinant for cure is resectability of lesion. Antifungal therapy alone is not associated with improved survival. The current recommendation is a combination of total surgical excision followed by systemic antifungal therapy. [1] Amphotericin B, flucytosine, itraconazole have been used with varying success in Cladophialophora bantiana brain abscess. The use of liposomal amphotericin B has been suggested as a way to increase the dose of amphotericin B while reducing its toxic effects, particularly nephrotoxicity. In vitro data suggest that itraconazole, voriconazole, and amphotericin B have activity against C. bantiana , with the azoles having lower MICs than amphotericin. [2] A newer azole, voriconazole was found effective in various in vitro studies. It has good penetration in CSF and brain tissue in comparison to itraconazole which do not have good CSF penetration. Voraconazole acts by inhibiting ergosterol biosynthesis which is an integral component of fungal cell wall. [10] However, even voriconazole along with liposomal amphotericin B could not save the patient in some of the cases. [11] Also, the high costs of these drugs and the prolonged duration of antifungal therapy are some of the issues that must be considered by the treating team, especially in the Indian subcontinent. We report a mortality in a patient who was immunocompetent and underwent a documented total microsurgical excision. He had, perhaps, the best chance of surviving this invasive fungal mycosis. It remains to be speculated whether this patient could have been salvaged if he had been given the benefit of Voriconazole and liposomal Amphotericin B from the very outset. However the cost of therapy would have approximately amounted to Rs. 3,00,000 (Amphotericin B) and a further Rs. 3,00,000 (Voriconazole). It is also clear that despite the clearly prohibitive cost of Rs 6,00,000, we as the treating team would not have been able to guarantee survival with even a reasonable degree of confidence. There is undoubtedly a need for further research to find out a novel cost-effective antifungal agent to which Cladophialophora bantiana is uniformly sensitive. Only then will an invasive CNS fungal mycosis be considered less deadly than a Glioblastoma multiforme- the most aggressive form of brain cancer which, in contrast, is still associated with a reasonable median survival exceeding eight months References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08085f6.jpg] [mb08085f3.jpg] [mb08085f2.jpg] [mb08085f1.jpg] [mb08085f4.jpg] [mb08085f5.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}