 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
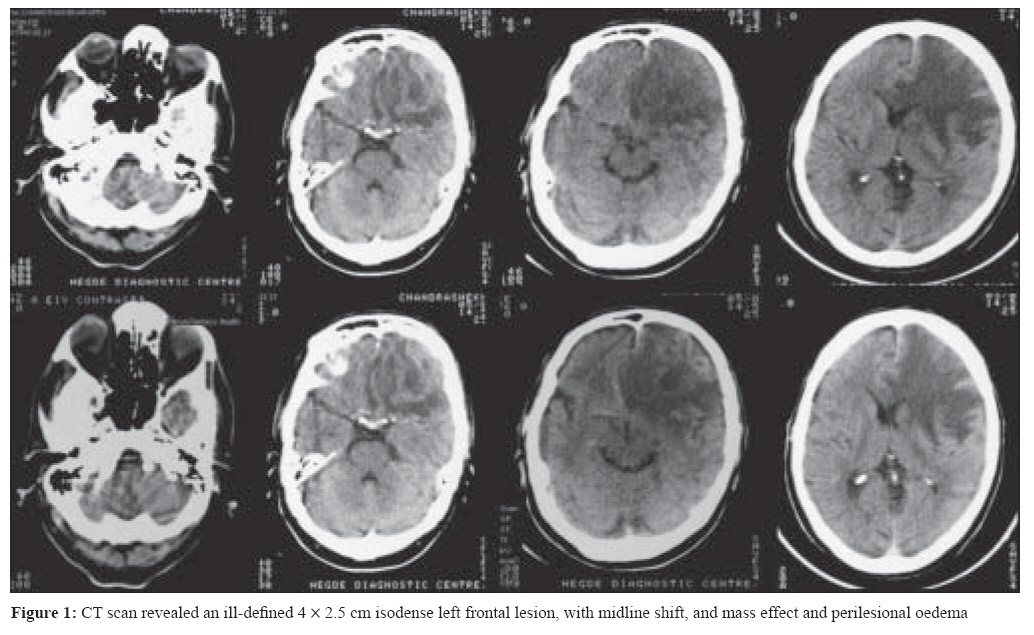
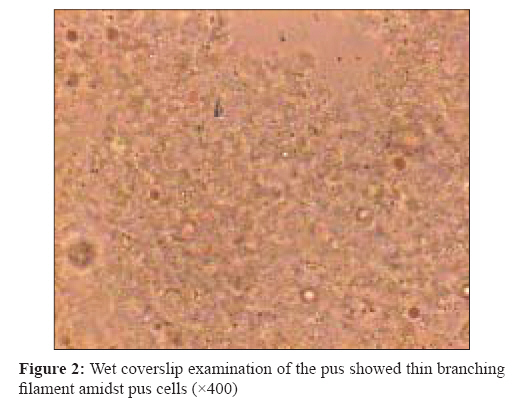
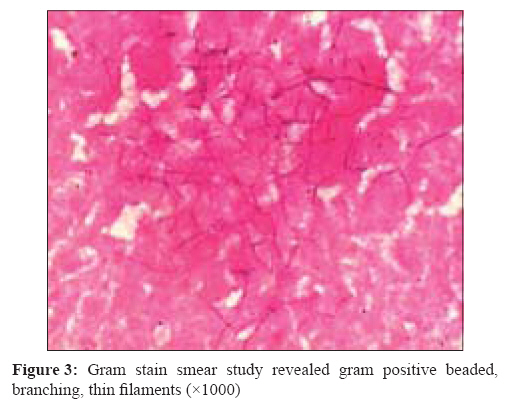
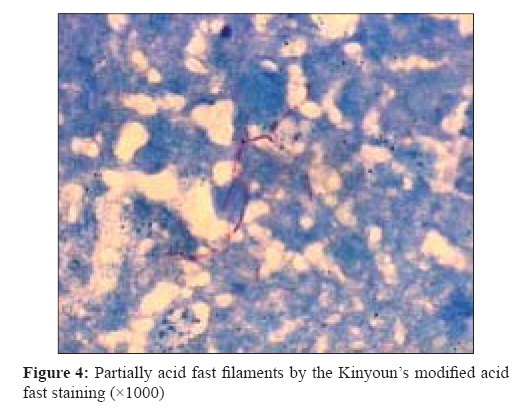
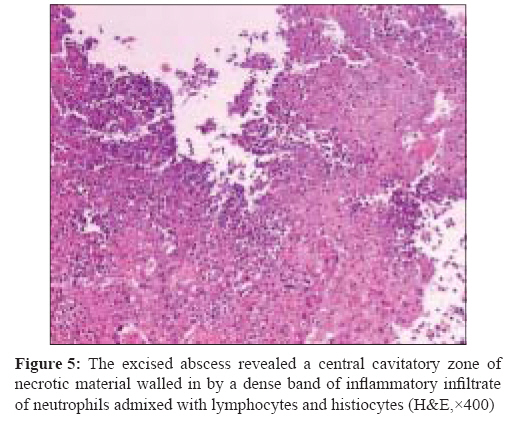
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 274-277 Case Report Nocardial brain abscess in an immunocompetent host Dias M, Nagarathna S, Mahadevan A, Chandramouli BA, Chandramuki A Department of Microbiology, St. John's Medical College, Bangalore-560 034, Karnataka Date of Submission: 12-Dec-2007 Code Number: mb08086 Abstract Nocardial infection of the central nervous system is rare and usually manifests as brain abscess. Here we describe an elderly gentleman who presented with signs and symptoms of an intracranial mass lesion localising to the frontal lobe. Clinical examination and CT scan suggested neoplasia as the probable diagnosis. A biloculated abscess was seen at surgery. Aspiration of the contents and examination of pus revealed Nocardia asteroides . Treatment included total excision and prolonged antibiotic therapy which resulted in an excellent outcome. Keywords: Brain abscess, intracranial mass lesion, Nocardia asteroides Nocardiae are aerobic catalase positive nonmotile gram variable to gram positive, acid alcohol fast branching filamentous bacteria belonging to Actinomycetales . [1] Infection usually occurs through inhalation or direct cutaneous inoculation. Primary infection is pulmonary or cutaneous. Haematogenous spread to the nervous system occurs and the characteristic lesion is an abscess which is usually poorly encapsulated. [2] Cerebral nocardiosis is an uncommon clinical entity, representing only 2% of all cerebral abscesses. [3] They rarely affect the central nervous system and manifest as brain abscesses. [2] Mortality is high especially in immunocompromised hosts. [2],[3] Paucity of clinical and laboratory signs of infection and insidious manifestations makes diagnosis and management difficult. Case Report A 67-year-old gentleman farmer from Haveri in Karnataka who was not a known diabetic or hypertensive, presented with history of headache and vomiting of six months, dry non productive cough and low grade fever of one month and speech disturbances of eight days duration. On clinical examination he was drowsy, with motor aphasia and bilateral papilloedema. Examination of the respiratory system, abdomen and cardiovascular system were unremarkable. Clinical suspicion was that of a space occupying lesion in the left posterior frontal lobe. Radiological diagnosis was glioma or metastasis. Provisional clinical diagnosis, considering the age of the patient and chronic history was glioma of posterior frontal lobe. Total white cell count was 12,000 cells/cmm; random blood sugar was 234 mg% and urine ketones were negative. Chest X-ray and abdominal ultrasound were normal. Patient was seronegative for HIV antibodies. A CT scan of the brain revealed an ill defined 4 x 2.5 cm isodense left frontal lesion, with midline shift, and mass effect and perilesional edema, suggestive of glioma or metastases [Figure - 1]. Treatment plan was craniotomy and excision of the tumour. Oral hypoglycaemic agent (daonil) was started for the elevated blood sugars. At surgery, a biloculated thick walled abscess containing 30 mL thick, mucoid, non foul smelling pus was seen extending till the basal frontal region. The pus was aspirated along with total excision of the abscess. Wet coverslip examination of the pus showed thin branching filament amidst pus cells [Figure - 2]. Gram stain smear study revealed gram positive beaded, branching, thin filaments [Figure - 3] which were partially acid fast by the Kinyoun′s (1% H 2 SO 4 ) modified acid fast staining [Figure - 4] suggestive of Nocardia spp. Growth was obtained aerobically on 5% sheep blood agar after 48 hours of incubation. The colonies were 2-3 mm in diameter, wrinkled with irregular margins and an earthy odour. Good growth was also obtained on Lowenstein Jensen medium after 48 hours which showed growth of granular, wrinkled colonies that turned orange at the end of one week. On SDA, initially off-white rough, heaped up colonies turned orange at the end of one week. Smears from culture showed gram positive to gram variable beaded filaments and coccobacillary forms which were also partially acid fast. Biochemical reactions were done for identification of species. Catalase test was positive, oxidase test negative, aesculin was hydrolysed, nitrate was reduced to nitrites and urease was positive. Casein hydrolysis, L-tyrosine hydrolysis and xanthine hydrolysis were negative. Citrate was positive. Good growth was obtained on incubation at 45°C. Antibiotic susceptibility pattern was as follows, gentamicin (10μg) sensitive, tobramycin (10μg) resistant, amikacin (30μg) sensitive, erythromycin (15μg) resistant. Based on these biochemical reactions and antibiotic susceptibility pattern, the isolate was identified as Nocardia asteroides. [1],[4] Blood cultures remained sterile even on repeated culture. Culture of sputum was negative for Nocardia . On histopathological examination, the excised abscess revealed a central cavitatory zone of necrotic material walled in by a dense band of inflammatory infiltrate of neutrophils admixed with lymphocytes and histiocytes. The necrotic centre was walled in by a zone of granulation tissue with proliferating vascular channels and fibroblasts. External to it was a collagenised capsule with hypertrophic reactive astrocytes at its junction adjoining the brain parenchyma. Special stains failed to reveal any fungal stain or bacteria [Figure - 5]. Postoperatively, the patient received empirical antibiotics (cefotaxime, amikacin, metronidazole) intended to cover bacterial abscess. After culture confirmation it was modified as per in vitro antibiotic susceptibility (Kirby Bauer method) to include cotrimoxazole. The patient was discharged on the seventh post operative day on cotrimoxazole for three month and advised follow-up. The patient was followed up with CT scan for one year at regular intervals and is doing well to date with no signs of recurrence or other complications. Discussion Nocardial infections are commonly encountered in immunocompromised states including HIV, alcohol abuse, alveolar proteinosis, diabetes mellitus, neoplasias and organ transplants. [2],[5] Nocardial lesions in lungs or elsewhere in the body frequently erode the blood vessels and once blood-borne, it disseminates to involve other sites. [2],[3] The hallmark of nocardial lesions is abscess formation and in the CNS, abscesses involving cerebrum, deep nuclear structures and cerebellum are seen [2] and often mimic brain tumours. [6] Spinal abscesses, meningitis and intracranial aneurysm have also been described due to this bacteria. [7],[8] The most common presentation is with evidence of progressively expanding intracerebral mass lesion which can be multiple or single. Nocardial brain abscesses are often misdiagnosed as malignant brain tumours [6] and a definitive diagnosis may not be possible without detecting bacteria from the lesion. Infection of the brain by Nocardia are often insidious in onset, difficult to diagnose and treat successfully. It is also associated with a high mortality rate, which has been considerably reduced with advent of the CT scan. [3],[8] Treatment consists of surgical management which includes abscess drainage and institution of appropriate antimicrobials after culture confirmation. [6],[9],[10] Cotrimoxazole remains the antibiotic of choice and duration of treatment varies from six weeks to one year. [3],[8] Although CNS nocardiosis is usually a consequence of pulmonary nocardiosis, no clinically evident pulmonary infection or other focus of infection could be found in this patient. Diabetes, which was detected incidentally on presentation, was probably the predisposing cause. Positive predictors include early diagnosis, absence of systemic nocardiosis, absence of co-morbid diseases and appropriate antibiotics. [2],[5] Complete surgical removal and prolonged antimicrobial therapy is required to prevent relapse of the infection. In this patient also, an early diagnosis with help of smear examination and culture confirmation made institution of appropriate antibiotic possible. Excellent patient compliance, regular follow-up and, absence of co-morbid factors helped in cure and prevented relapse in this patient. This case emphasises the propensity of nocardial infections to mimic other conditions, particularly malignancy, which may lead to delay in appropriate surgical treatment and antimicrobial therapy with serious consequences. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08086f1.jpg] [mb08086f4.jpg] [mb08086f2.jpg] [mb08086f5.jpg] [mb08086f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}