 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
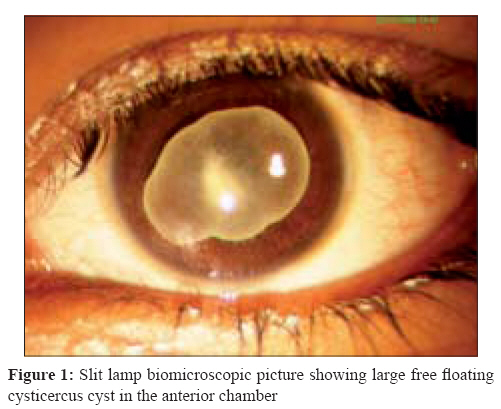
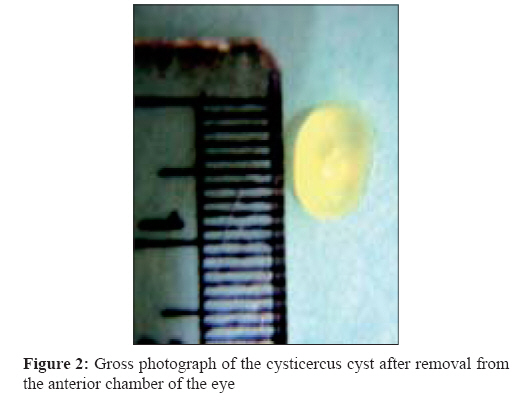
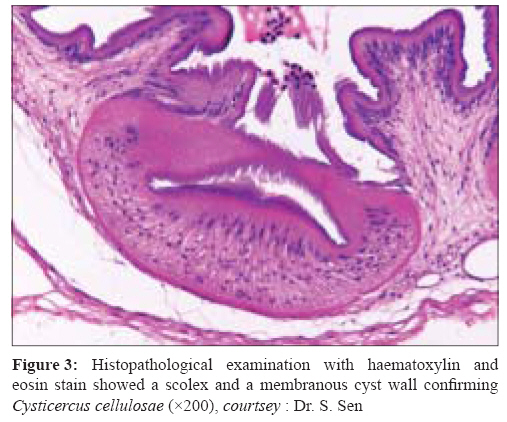
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 277-279 Case Report Viscoexpression of large free floating cysticercus cyst from the anterior chamber of the eye by double incision technique Kai S, Vanathi M, Vengayil S, Panda A Dr. R P Centre for Ophthalmic Sciences, All India Institute of Medical Sciences, New Delhi - 110 029 Date of Submission: 13-Jan-2008 Code Number: mb08087 Abstract We describe a case of 16-year-old girl who reported with diminution of vision in left eye for past seven months with appearance of white reflex. Slit lamp biomicroscopy revealed the presence of a live grayish white cyst in the anterior chamber. The ultrabiomicroscopic evaluation revealed a large live Cysticercus cellulosae cyst in anterior chamber. The CT-scan of the brain revealed multiple non-contrast enhanced lesions with calcification in brain parenchyma. The patient was started on oral prednisolone and oral albendazole. The cyst was removed in toto from the eye by double incision technique. The patient achieved visual acuity of 6/12 post-operatively.Keywords: Cysticercus in anterior chamber, double incision technique, ocular cysticercosis Cysticercosis is caused by the parasite Taenia solium . Man is intermediate host and it is transmitted to humans by faeco-oral route. The larvae migrate to various parts of body via lymphatics and blood. They may develop in any organ of the body and the clinical manifestation depends upon the target tissue involved. Ocular involvement occurs in 46% of the infected patients. Ocular cysticercosis can involve the ocular adnexa, the subconjuctival space and both anterior and posterior segment of the eye. The subretinal space is considered to be the most common site for ocular cysticercosis, [1] though some authors have reported the subconjuctival space to be the most common site. The presenting clinical features such as recurrent conjunctivitis, conjuctival swelling, proptosis, defective vision depend on the site of ocular involvement. Anterior chamber cysticercosis is unusual. [2] The management is mainly surgical. Various surgical modalities described include paracentesis, extraction with capsule forceps, cryoextraction, erysiphake extraction and viscoexpression. [2] We report a case of a large live cysticercus cyst in the anterior chamber of the eye with asymptomatic neurocysticercosis. The cyst was removed by visco expression from anterior chamber of the eye. Case Report A 16-year-old female patient reported in May 2007 to our out-patient department with the history of diminution in her left eye for past seven months associated with appearance of white reflex in left eye for four months. She had no history of other ocular complaints such as pain, watering, discharge, proptosis or diplopia or any systemic complaints such as fever, headache, or seizures. There was no history of any surgery done on her both eyes. The patient was vegetarian and did not have any pets. The patient had corrected visual acuity of 6/6 in right eye and 1/60 in left eye. On torch light examination a whitish cystic structure covering the pupillary area in left eye anterior chamber was seen. The intraocular pressure was normal in both the eyes. Slit lamp biomicroscopic examination of the left eye revealed the presence of a live greyish white cyst in the anterior chamber [Figure - 1]. There were fluorescent green dots on the outer wall of the cyst all around. The fluid wave movements could be seen in the cyst and it was found to alter its shape and size. The cyst was not attached to the cornea but its underlying relation with the iris and crystalline lens could not be appreciated on slit-lamp examination. The anterior chamber angles were free from cyst and there was no inflammatory reaction in anterior chamber. The indirect ophthalmoscopy was not possible in the left eye and that of the right eye was normal. The ultrasonographic evaluation for involvement of the orbit and ocular adnexa including all recti muscles was normal. The ultrabiomicroscopic (UBM) evaluation of the left eye revealed a large live cyst in anterior chamber with movements of the fluid and alteration in the shape. The CT-scan of the brain revealed multiple non-contrast enhanced lesions with calcification in brain parenchyma. We made the presumptive diagnosis of ocular cysticercosis with asymptomatic neurocysticercosis. The patient was started on oral prednisolone (1 mg/kg) and oral albendazole (15 mg/kg). She was also started on topical steroid and antibiotic drops. Under peribulbar anaesthesia, a self sealing side stab incision was made at 12 o′clock position with a MVR blade and extended to 1.5 mm. Movement of the cyst towards the incision despite use of ocular viscoelastic device (OVD-methylcellulose) to push the cyst away from the incision site prompted us to make another clear corneal entry temporally at the 3 o′clock position with a 3.2 mm keratome. Then OVD was injected into the anterior chamber through the superior incision, simultaneous decompression of the anterior chamber by pressing down on the posterior lip of the temporal incision allowed the cyst to engage in the temporal incision. Further slow decompression of the chamber of the superior wound facilitated total extrusion of the cyst from the anterior chamber without rupture. The incision wound was sutured with 10.0 monofilament suture. The superior wound was closed by hydration. On gross examination, the cyst was greyish white with dimensions 0.8 cm x 0.5 cm [Figure - 2]. The cyst was fixed in 10% formalin and stained with haematoylin and eosin. Histopathological analysis showed a scolex with double row of hooklets and a membranous cyst wall suggestive of Cysticercus cellulosae [Figure - 3]. Postoperatively topical and systemic treatment was continued. The patient achieved visual acuity of 6/12 postoperatively. Detailed fundus examination of left eye after dilatation was normal and no other anterior and posterior segment abnormalities were detected. Discussion Cysticercosis is endemic in India and contributes to preventable blindness. [3] It can have a varied presentation. The ocular entry by cysticercus cyst is usually through posterior ciliary arteries [1] and that involving the vitreous cavity and optic nerve [4] can result in vision loss. Presentation of free floating live cyst in anterior chamber is a much rarer occurrence. [2],[5],[6] The route of entry to anterior chamber is debatable. It can enter the anterior chamber from the posterior segment through pupil in aphakes, [6] anterior chamber angle or through vessels feeding ciliary body. The clinical diagnosis of live intraocular cysticercosis is based on the morphology of the parasite as visualized with the ophthalmoscope or slit lamp biomicroscope. The cyst shows characteristic movements-undulating, contracting and expanding; the scolex (when evaginated) may make pendulous movements. When the scolex is invaginated, its location within the cyst is indicated by a dense white spot called the receptaculum capitis. Laboratory studies are of limited value in intraocular cysticercosis. Eosinophilia is usually absent unless there is widespread dissemination of the parasite. Serological tests lack sensitivity. [7] The indirect haemaggultination test shows cross reactivity between cysticercosis and echinococcosis. Evidence of intenstinal Taenia solium is seldom found in human cysticercosis. In our case, the absence of any reaction in anterior chamber, normal iris and crystalline lens and free anterior chamber angles indicated that the most probable route of entry was via vessels supplying the ciliary body. Irrespective of the pathogenesis, removal of the cyst intact and safely from the anterior chamber without damage to adjacent structure is of utmost importance. Breach in the integrity of the cyst in the anterior chamber can incite severe inflammatory reactions, induce cataract formation and cause toxic damage to the optic nerve too. Our case reports the presence of a large live free floating cysticercus cyst in the anterior chamber in a young patient with asymptomatic neurocysticercosis and highlights its in-toto removal. Various surgical modalities include paracentesis, extraction with capsule forceps, cryoextraction, erysiphake extraction and viscoexpression. [2] Viscoexpression requires minimal tissue manipulation and working space. Owing to the large size of the cyst and minimal space available in the anterior chamber we opted to remove the cyst by viscoexpression technique. Beri et al , [2] have described the removal of an anterior chamber cyst by viscoexpression through a single 3 mm supero-temporal incision. A single entry to remove the cyst in our case was difficult as the cyst was too large filling most of the anterior chamber. The cyst was also found to move towards the incision soon after entry, thereby preventing our attempts to enlarge the entry incision as we feared the risk of rupture of the cyst on possible contact with the MVR blade. We therefore adopted a double entry method for viscoexpression of the large cyst. It is interesting to note that a cysticerus cyst as large as to fill almost three-fourths of the space of the anterior chamber, as in our case, was able to squeeze itself through a clear corneal tunnel wound of 3.2 mm with facilitation of decompression through assistance from the superior entry wound. We recommend this double incision technique for successful in toto removal of large cysticercus cysts from the anterior chamber. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08087f2.jpg] [mb08087f3.jpg] [mb08087f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}