 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
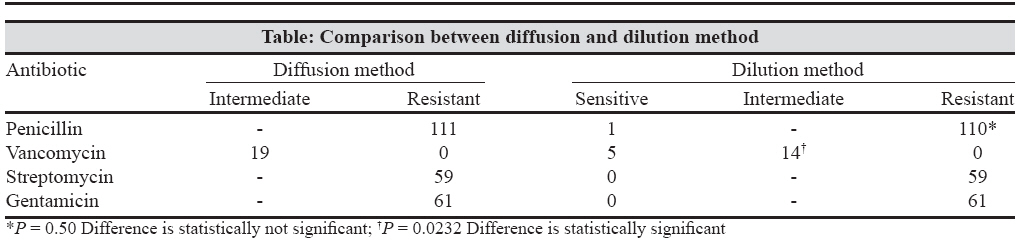
Indian Journal of Medical Microbiology, Vol. 26, No. 3, July-September, 2008, pp. 285-287 Correspondence Study of antimicrobial resistance in enterococci Rahangdale VA, Agrawal G, Jalgaonkar SV Department of Microbiology, Indira Gandhi Government Medical College, Nagpur - 440 018 Date of Submission: 03-Oct-2007 Code Number: mb08093 Dear editor, Enterococci are important causes of both community acquired and nosocomial infections. They show intrinsic resistance to a number of commonly used antibiotics, particularly the cephalosporins. During the last few years, enterococci have acquired resistance to a number of important antibiotics including glycopeptides. [1] Enterococci resistant to all three antimicrobial agents (penicillin, aminoglycosides and vancomycin) pose a serious challenge not only for clinicians but also for health care institutions. It results in treatment failure, selection and spreading of resistant strains in the health care institution. Imprudent use of antibiotics and colonisation pressure are the important causes of the drug resistance in enterococci. [2] In vitro testing of antimicrobial susceptibility of all clinical enterococcal isolates, suitable modification of the usual susceptibility testing procedures, judicial use of antibiotics, systematic surveillance and control of faecal colonisation of resistant enterococci in hospital staff are some of the measures to be adopted for control of the drug resistance in enterococci. [3] The objective of the present investigation was to study the antibiotic resistance in clinical isolates of enterococci. Enterococcal isolates from clinical samples from Indira Gandhi Government Medical College and Hospital, Nagpur, India were studied. Written consents of patients were taken to use their results in a published study. Enterococcal strains were subjected to Kirby-Bauer disc diffusion method as per the National Committee of Clinical Laboratory Standards (NCCLS) guidelines 2002. [4] Isolates found resistant or intermediate resistant to penicillin G, vancomycin, gentamicin or streptomycin were processed for determination of minimum inhibitory concentration (MIC) by agar dilution method. [4] Strains which were sensitive to penicillin or ampicillin were tested for β lactamase production. [5] A total number of 123 enterococcal strains were included in the study, of which 79(64.23%) were E. faecalis , 40(32.52%) E. faecium , 3(2.44%) E. gallinarum and 1(0.81%) E. raffinosus . The higher frequency of E. faecalis infection might be due to its greater intrinsic virulence. The enterococcal strains intermediate resistant or resistant to penicillin, vancomycin, streptomycin and gentamicin by diffusion method were subjected to the dilution method [Table - 1]. Fischer Exact test was applied to compare the findings of the two tests. Good correlation was seen between two methods for penicillin, streptomycin and gentamicin. Out of the total 111 enterococcal strains found resistant to penicillin by diffusion method, only one was found sensitive by dilution method (difference was not statistically significant). There was complete correlation between two methods for gentamicin and streptomycin. Out of 19 enterococcal strains found intermediate resistant to vancomycin by diffusion method, 5 were found sensitive by dilution method ( P < 0.05)). Because of the error associated with disc diffusion susceptibility testing, its use might result in unwarranted elimination of the antibiotic as a part of possible treatment regimen. Therefore, the susceptibility tests that detect vancomycin resistance accurately must be used for vancomycin resistant enterococci (VRE) determination. NCCLS [4] recommends the dilution test for VRE determination. Penicillin resistance has increased in the recent years. In the present study, 110 (89.43%) enterococcal strains showed penicillin resistance and 47 (38.21%) strains were having MIC as high as 256 μg/mL. Because penicillin is a mainstay of therapy for infections due to enterococci, the organism′s development of high level resistance to this drug would have important clinical implications. NCCLS [4] designates penicillin and ampicillin as comparable agents that need not be duplicated in antimicrobial susceptibility testing. In the present study, there were total 110 (89.43%) isolates resistant to penicillin, of which 54 (43.90%) isolates were resistant to both penicillin as well as ampicillin. Remaining 56 enterococcal strains, which were penicillin resistant were sensitive to ampicillin. As against NCCLS [4] guidelines with our observation, penicillin and ampicillin should be tested separately. None of the penicillin and ampicillin susceptible strains was found to produce beta-lactamase. Vancomycin resistance is low in our region (11.38% intermediate resistance in present study) which is also reported by other Indian studies [2] in contrast to reports from USA, [1] where vancomycin resistance is more common. In our study, about 10 (8.13%) of enterococcal strains showed raised MIC of 16 μg/mL for vancomycin. The last therapeutic resort for enterococci was vancomycin. Unfortunately, recently VRE have taken firm hold and have become epidemic in some hospitals and regions. Streptomycin and gentamicin resistance in the present study is 47.96% and 49.59% respectively, which is alarmingly high percentage of resistance and is worthy of note. Combination therapy with cell wall active agent (penicillin, ampicillin or vancomycin) and an aminoglycoside (gentamicin or streptomycin) was recommended for the treatment of serious enterococcal infections. But high level resistance to aminoglycoside could however, nullify the efficacy of this combination. Therefore, to distinguish these high level aminoglycoside resistant strains from simply intrinsic resistant strains is of vital importance. Hence, we have tested for high level resistance to aminoglycosides by dilution method. There were total 11 enterococcal isolates which were resistant to both the tested aminoglycosides but fortunately all of them showed HLGR but not HLSR. All these 11 isolates were E. faecium . Most enterococcal infections observed in non-immunocompromised hosts can be treated with a single antibiotic. Penicillin, ampicillin remain the drug of choice. A glycopeptide antibiotic is the alternative agent. Combination of a cell wall active agent (penicillin or glycopeptide) plus an aminoglycoside will improve the outcome of enterococcal infections, particularly that of serious infections, such as meningitis and endocarditis. Infections resulting from glycopeptide-resistant enterococci are among the most difficult to treat. NCCLS 2002 suggested various drugs for enterococci and VRE. In the present study, 100% sensitivity to linezolid was observed. Pristinomycin also has good susceptibility (92.43%), but it can be used for E. faecium infections only. They may be of utmost utility for multidrug resistant strains. Other suggested options for VRE are chloramphenicol, erythromycin, tetracycline and rifampicin. Except chloramphenicol, other antibiotics showed high resistance in our study. Nitrofurantoin and ciprofloxacin alone are limited for the treatment of urinary tract infection including prostatitis. Only 22.76% of strains were resistant to nitrofurantoin. There was good sensitivity for gatifloxacin (88.61%) and fosfomycin (97.47%). In the present study, E. faecium was found more resistant to commonly used antienterococcal drugs as compared to E. faecalis , which was also reported by Karmarkar et al . [2] Multiple drug resistance was observed in enterococci, more so in E. faecium . A total of 95 (77.23%) enterococcal isolates showed resistance to six or more than six drugs. In conclusion, multi-drug resistant enterococci have become a serious threat to public health. Enterococci with raised MIC to penicillin and high level resistance to aminoglycosides are being reported. Although the incidence of vancomycin resistance was low, its presence is a cause of concern. It is important to maintain regular surveillance of antibiotic susceptibilities so that changes in their pattern can be detected early. References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08093t1.jpg] |
| |||||||||
{kind=link}