 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
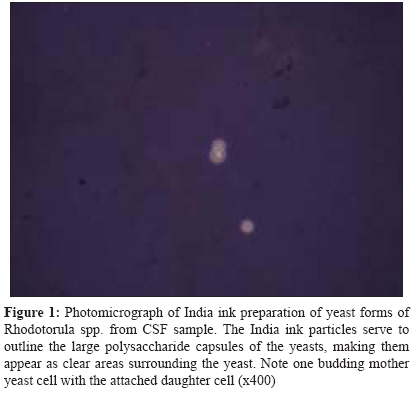
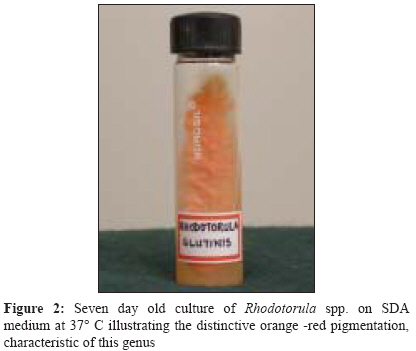
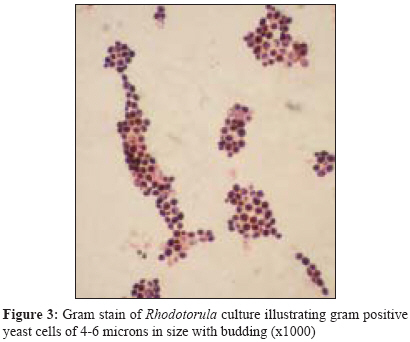
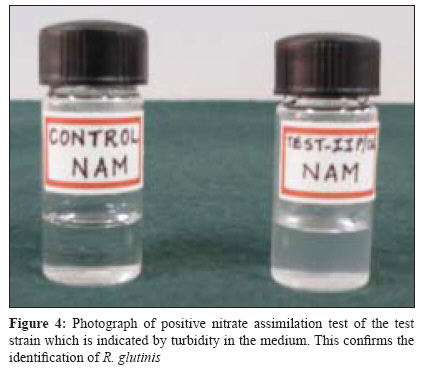
Indian Journal of Medical Microbiology, Vol. 26, No. 4, October-December, 2008, pp. 375-377 Case Report Meningitis due to Rhodotorula glutinis in an HIV infected patient Shinde RS, Mantur BG, Patil G, Parande MV, Parande AM Department of Microbiology, Belgaum Institute of Medical Sciences, District Hospital Compound, Belgaum - 590 001, Karnataka Date of Submission: 27-Mar-2008 Code Number: mb08114 Abstract Rhodotorula spp, though considered a common saprophyte, recently has been reported as causative agent of opportunistic mycoses. We present a case of meningitis in an immunocompromised human immunodeficiency virus infected patient who presented with longstanding fever. He was diagnosed as a case of chronic meningitis. Diagnosis was confirmed by cell cytology, India ink preparation, Gram staining and culture of cerebrospinal fluid (CSF) sample. CSF culture grew Rhodotorula glutinis . Therapy with amphotericin B was successful in eliminating the yeast from CSF and the patient was discharged after recovery.Keywords: Human immunodeficiency virus, meningitis, rhodotorula. The yeast Rhodotorulae are members of the family Cryptococcaceae , subfamily Rhodotorulodeae. Of the various species of Rhodotorula, Rhodotorula glutinis and Rhodotorula rubra (mucilaginosa ) are the most common. [1] Rhodotorula species are common saprophytes in the environment and usually found in the skin, lungs, urine and faeces. Like other yeast and yeast - like organisms, Rhodotorula was considered as a non-virulent saprophyte till recent times. Rhodotorula spp. have been implicated as a cause of meningitis, endocarditis, ventriculitis, peritonitis, fungaemia, central venous catheter infection and keratitis. [2] Meningitis due to Rhodotorula is relatively uncommon, with only few cases reported in the literature. [1],[3],[4],[5] Here, we report a case of meningitis due to Rhodotorula glutinis in an human immunodeficiency virus (HIV) infected patient which is still rarer as it is the second case reported till now. Case Report A 35-year-old HIV seropositive male, was admitted on 15 May, 2007 with history of high grade, evening rise temperature, associated with chills and rigors since six months. This was aggravated since three days. The patient also complaints of neck pain, headache and vomiting since three days. On general examination, the patient was found to be febrile (101 0 F), malnourished and cachectic with marked pallor. His body mass index (BMI) was found to be 16 which was below 18.5-24.9, the normal range of BMI for the Indian population. Central nervous system examination revealed altered sensorium but no clear meningeal signs were observed. With above clinical history and physical examination patient was provisionally diagnosed as a case of chronic meningitis with immunocompromised status. Complete haemogram and blood chemistry revealed- Hb-7gm%, ESR- 130 mm at the end of one hour, total leukocyte count (TLC) -10,450/cmm, blood glucose - 71 mg/dL, Urea-19.5 mg/dL, creatinine- 1.4 mg/dL. Urine analysis and x-ray chest were normal. Lumbar puncture was performed under aseptic precautions and cerebrospinal fluid (CSF) collected in a sterile container. CSF was subjected to cell cytology examination, biochemical analysis, India ink preparation, Gram staining and cultural studies. [6] Cell cytology revealed WBC count of 40 cells/cmm with all lymphocytes, CSF protein content was 33.2 mg/dL and sugar was 43.3 mg/dL. India ink preparation of CSF showed encapsulated budding yeast cells [Figure - 1], Gram stain of CSF showed round, budding yeast cells of 4-8 μm in diameter with clear halo around the cells, with occasional inflammatory cells. Patient was retested for HIV antibodies using Comb- Aids (Span diagnostics), Capillus (Trinity biotech) and Tri-dot (J. Mitra) after counselling and found reactive to HIV-1 antibodies. A presumptive diagnosis of cryptococcal meningitis was made on the basis of India ink preparation and Gram staining. The empirical antifungal therapy with amphotericin (0.7 mg/kg/day) was started. On the third day, CSF culture results were obtained. Routine bacteriological cultures of CSF did not grow any organism, whereas Sabouraud dextrose agar at 37 o C and 20 o C revealed growth of Rhodotorula spp. which was identified by its colony morphology. Colonies were moist, glistening, smooth to mucoid and of salmon pink to coral red colour [Figure - 2]. Gram staining of the growth revealed budding yeast cells which were short, ovoid, 2 to 6.5 μm in diameter and arranged in short chains and clusters [Figure - 3]. Two more samples revealed the same findings. Further inositol assimilation and nitrate assimilation tests were carried out using Wickerham broth medium. These tests were used to differentiate Rhodotorula spp. from C ryptococcus spp. and were also used for speciation. [7] Tubes of yeast nitrogen base without inositol and yeast carbon base without potassium nitrate were prepared and used as controls to check "carry over" of nutrients that may have been stored within the yeast cells when grown on the previous medium. Rhodotorula suspension of McFarland # 1 standard was inoculated into inositol assimilation medium and nitrate assimilation medium. Test strain was negative for inositol assimilation test and was able to assimilate nitrate hence was confirmed as Rhodotorula glutinis [Figure - 4]. The patient was continued on antifungal treatment and was discharged after 20 days of hospitalization after recovery. Discussion Members of Rhodotorula species are generally considered to be non pathogenic and have rarely been a cause of infection in humans. They are commonly recovered from human skin, lungs, conjunctivae, urine and gastrointestinal tract. [8] The genus Rhodotorula is a pigmented yeast classified under the family Cryptococcaceae and includes 38 species. Rhodotorula rubra is most commonly isolated from clinical specimen followed by R. glutinis. Rhodotorula species produce moist, smooth to mucoid, glistening, pigmented colonies. Salmon-pink to coral red colour of the colony is attributed to the carotenoid pigment, torularhodin. [8] Rhodotorula spp. and Cryptococcus spp. have many similar morphological and physiological properties and have been mistaken for each other. Rhodotorula spp. differs from Cryptococcus spp. by its inability to assimilate inositol and its carotenoid pigment. [8] Though it is a saprophyte, its isolation from blood cultures and other sterile fluids such as CSF is of greater significance when contamination is ruled out. [9] Rhodotorula is increasingly being identified as a human pathogen. [8] Rhodotorula spp. have been implicated as a cause of meningitis, endocarditis, ventriculitis, peritonitis, fungaemia, central venous catheter infection and keratitis. [1],[2],[3],[4],[5],[8],[10] Relapse with Rhodotorula species is not known except one case of recurrent catheter infection and one case of meningitis. [3],[8] In general, Rhodotorula spp. seems to have lower virulence in comparison to other yeast, with about 15% mortality overall. [8] However, infection can occasionally be a life threatening complication, particularly in immunocompromised individuals. Fatal cases of Rhodotorula meningitis or meningoencephalitis and sepsis have been well documented by autopsy findings. [8] To the best of our knowledge there are only four case reports about Rhodotorula meningitis, out of which three are due to R. rubra and one is due to R. glutinis . [1],[3],[4],[5] Here we report the second case of R. glutinis causing meningitis. Of the four patients, only one patient was immunocompetent, [1] two were immunocompromised due to HIV infection, [3],[4] and one was suffering from leukemia. [5] Fever was the common symptom in most cases. In our case too, fever was the prominent symptom with HIV as the predisposing factor. Neurological manifestation like altered sensorium was noted in our patient along with the presence of cytological parameters. Positive India ink preparation and isolation of Rhodotorula on Sabouraud dextrose agar confirmed the clinical findings of meningitis with Rhodotorula spp. Rhodotorula spp. infection can be successfully treated with amphotericin B, 5 fluorocytosine (5 - FC) and azoles like itraconazole. [2] Relapse with Rhodotorula meningitis was reported by Gyaurgieva et al, [3] which was successfully treated with suppressive therapy with itraconazole followed by maintenance therapy. Our patient also responded to amphotericin B and was discharged after recovery. In conclusion, immunocompromised patients especially those with HIV, leukemia and those receiving broad spectrum antibiotics are susceptible to infections with Rhodotorula spp.. Infection by these rare yeast could be under reported because it is often mistaken for C. neoformans on microscopy and often considered as a sample contaminant. Hence routine culture of all positive India ink preparations should be carried out to prove the pathogenic role of these rare yeasts. Acknowledgement We thank Dr. Satish K. Amarnath, Medical Director from Manipal Cure & Care, Bangalore, India, for critical reviewing of the manuscript.References
Copyright 2008 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb08114f1.jpg] [mb08114f3.jpg] [mb08114f4.jpg] [mb08114f2.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}