 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 17-21 Original Article Maternal and neonatal screening for Group B streptococci by SCP B gene based PCR: A preliminary study Elbaradie SaharMY, Mahmoud Manal, Farid Mona Department of Obstetrics and Gynecology, AlFayom University Date of Submission: 22-Feb-2008 Code Number: mb09004 Abstract Objective: To detect the magnitude of group B streptococcal (GBS) colonization and disease among a sample of pregnant women and their infants in Egypt.Study Design: Prospective observational study. Participants: The study included 95 pregnant females, 35-37 weeks of gestational age, attending the antenatal outpatient clinic at AlFayom University Hospital between September 2006 and June 2007. All participants were screened with vaginorectal swabs by a conventional GBS PCR assay. Participants were grouped into group A (GBS present, 17 patients) and group B (GBS absent, 78 patients). Details with regard to labor and delivery were recorded and placental pathology was examined to detect histological chorioamnionitis. Ninety-five infant data were also recorded. All neonates of group A (17 out of 95 with known positive maternal GBS) underwent collection of simultaneous specimens from surface sites for PCR before their first bath and within four hours of birth. Results: GBS carriage rate in the study sample was 17.89%. Chorioamnionitis confirmed in three patients by placental pathology (one was in group A and two in group B) was statistically not significant. Twenty-two women had rupture of membranes (<12 hours) before delivery (four from group A and 18 from group B) that was not statistically significant. There were three infants out of 17 in group A who had GBS colonized at one or more sites by PCR which was statistically significant. However, only one infant was admitted to neonatal intensive care unit (NICU) that was not statistically significant. Conclusion: Maternal GBS carriage is associated with a significant increase in neonatal infection rate but is not associated with an increase in neonatal intensive care admission. An accurate evaluation of colonization rate (using a larger sample) is desired to evaluate neonatal invasive disease and determine the cost effectiveness of PCR to select an appropriate preventive strategy in Egypt. Keywords: Chorioamnionitis, group B streptococcal, neonatal infection, PCR, premature rupture of membranes Group B Streptococcus (GBS) is a facultative Gram-positive diplococcus originally known for causing bovine mastitis and was not demonstrated to be a human pathogen until 1938. [1] In 1970s, GBS emerged as the leading cause of neonatal morbidity and mortality, with a frequency of 2-3 cases per 1,000 live births and case-fatality ratios as high as 50%. [2] It causes severe invasive infection in newborns, 80% of which occur within the first week of life (early-onset neonatal sepsis) that results from ascending spread of GBS into the amniotic fluid through both ruptured and intact membranes. [3],[4] Transmission from mother to child has been reported to be 29 times higher in GBS-colonized mothers than in noncolonized mothers. The prevalence of GBS colonization in the vagina and/or rectum among pregnant women can vary among ethnic groups and geographical locations, ranging from approximately 10-40%. Although GBS colonization is not associated with disease in healthy women, colonization in pregnant women may be associated with urinary tract infection, bacteremia, amnionitis, endometritis, postpartum wound infections, and rarely, meningitis. [5] A number of obstetric factors have been associated with an increased likelihood of early-onset GBS in the newborn. These include maternal colonization of the vagina and rectum with GBS, preterm birth, prolonged rupture of membranes, intrapartum fever, women younger than 20 years, women with prior GBS-infected infant, women with heavy colonization-GBS bacteriuria equal to or greater than 104 colony forming units or low levels of anti-GBS capsular antibody6. Intrapartum antibiotic prophylaxis (IAP) has been shown not only to interrupt the transmission of GBS from mother to infant but also to reduce the incidence of early-onset GBS disease. [7] Guidelines from the Federal Centers for Disease Control and Prevention (CDC), [8] the American College of Obstetricians and Gynecologists, [5] and the American Academy of Pediatrics [9],[10] recommend two different strategies for the selection of candidates for IAP: either screening for GBS vaginorectal carriers or identification of maternal clinical risk factors for early-onset neonatal GBS disease. They recommend obtaining rectovaginal cultures at 35-37 weeks of gestation with the culture-based approach. [8] The value and practicality of both strategies have been debated in literature. An issue is potential overtreatment (in the case of the culture strategy) and under treatment (in the case of the risk-factor strategy) of patients, as well as the associated cost. For example, the standard screening test, a rectovaginal culture taken at 35-37 weeks, has been controversial because it may not accurately predict genital tract colonization at the time of labor (with an estimated sensitivity of 87-91% and specificity of 89-96%). The risk-factor method, on the other hand, would target treating the mothers believed to be at greatest risk but would miss many colonized mothers and at-risk infants. [11] Despite their limitations, both approaches are effective in reducing early-onset GBS infection rate in infants, although more widespread implementation of the guidelines is needed. [7],[12] The Committee on Obstetric Practice recognized that compliance with the culture-based approach will require the implementation of several steps13
The sensitivity of cultures in detecting GBS colonization varies from 54-87%, and results has a slow turnaround time requiring up to 36-72 hours before results can be issued. [3],[14] Besides being time consuming, this method requires an experienced technician to identify the suspected colonies, which are not always beta-hemolytic. Moreover, the suppression of GBS growth by enterococci present in the vaginal and rectal flora could lead to false-negative results. [15] Rapid methods of detection of GBS colonization in pregnant women, namely molecular biology based assays have become the focus of investigation in recent years. The most promising of these techniques is the polymerase chain reaction (PCR), which is reported to be highly sensitive and specific among women in labor and to yield results in 30-45 minutes. [16] The rate of GBS colonization and disease among pregnant women and their infants have not been studied in Egypt, and preventive strategy has not been formulated with regard to IAP. The purpose of our study was to detect the magnitude of the condition in our community (preliminary study), improve and simplify the diagnosis of GBS infection for routine clinical practice, and to evaluate a rapid, reliable, easy-to-perform, and inexpensive test to detect antenatal GBS colonization in pregnant women. Materials and Methods Study design Prospective observational study. Participants The study included 115 pregnant females at 35-37 weeks of gestational age attending the antenatal outpatient clinic at AlFayom University Hospital between December 2006 and September 2007. All participants were screened by a conventional GBS PCR assay. Patients who were followed till delivery without prolonged rupture of membrane were eligible to enter the study (thirteen patients were lost to follow up and seven had prolonged rupture of membrane (>12 hours) and details with regard to labor and delivery were recorded in 95 patients (delivery was conducted at AlFayom General Hospital). Data of ninety five infants was also recorded. Study protocol After explaining the procedure and aim of the work, vaginorectal swabs were collected for detection of GBS, according to CDC recommendations. [10] For combined vaginal and anal samples, first a swab from the mucosal secretions of the lower-third part of the vagina was obtained. Thereafter, the same swab was carefully inserted approximately 2.5 cm beyond the anal sphincter and gently rotated to touch the anal crypts. The swabs were placed in Amies transport medium and sent to the microbiology laboratory for testing by conventional PCR assay. Participants were grouped into group A (GBS present) and group B (GBS absent). Obstetricians attending the delivery were blinded to the study and none of the women received IAP. Details with regard to labor and delivery were recorded in 95 patients (delivery was conducted at AlFayom General Hospital). These include clinical rupture of membranes, its duration, and the number of vaginal examinations. Maternal chorioamnionitis was defined clinically, based on the obstetrician′s documentation. Specific clinical signs, such as fever ≥38 °C, foul-smelling liquor or fetal tachycardia were recorded. Placental membrane pathology were also obtained to detect histological chorioamnionitis (mono- and polymorphonuclear leukocytic infiltrate of the chorion) and confirm its diagnosis. Data such as gestational age, gender, birth weight, results of diagnostic evaluation, Apgar score, and admission to neonatal intensive care unit were also recorded in ninety five neonates. In neonates of group A (maternal GBS present) swabs from both nares and both external auditory canals (a total of two) were collected before their first bath and within four hours of birth. They were immediately placed in Amies transport media and sent to the microbiology laboratory for isolation by PCR assay. PCR was performed on 34 samples. Conventional PCR on incubated LIM broth Swabs were placed into LIM, a selective enrichment broth (Todd Hewitt broth with 15 μg/ml nalidixic acid and 10 μg/ml colistin) and incubated overnight followed by freezing at -70 °C. Most of the molecular genetic procedures were carried out according to standard protocols. [17] Bacterial DNA from the clinical samples was prepared by the phenol/chloroform extraction as follows:
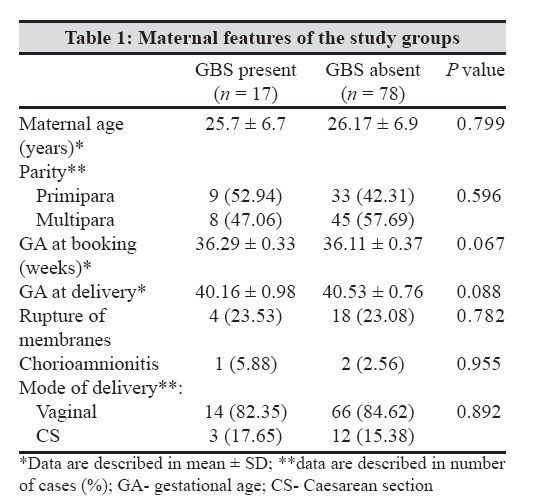
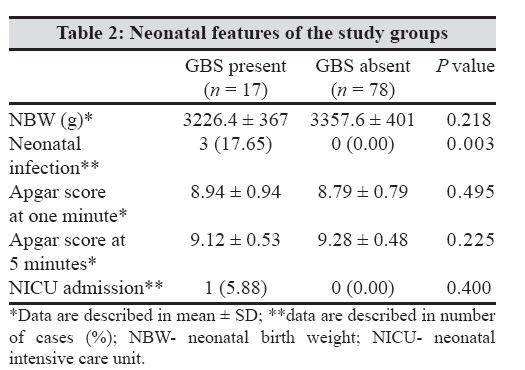
A lyophylized and noninfectious plasmid DNA acted as the internal control. PCR was performed using the primers: 5′-ACAACGGAAGGCGCTACTGTTC- 3′ (forward) and 5′ -ACCTGGTGTTTGACCTGAACTA- 3′ (reverse). These primers target the scp B gene that encodes C5a peptidase. Fifty microliters of the PCR mixture (20 mM Tris-HCl pH 8.4, 50 mM KCl, 2.5 mM MgCl 2, 0.4 mM each deoxynucleotide, 0.4 μM of each primer, 1 U Platinum Taq polymerase (Invitrogen), and internal control DNA, when needed) was added to the 22 μl DNA preparation. The PCR was performed as follows: Five minutes at 94 °C, 45 cycles of 30 secs at 94 °C, 30 secs at 55 °C, 30 secs at 72° C (thermocycler BE 9600). After electrophoresis (on 2% agarose gel) the sizes of DNA fragments were calculated using 100 bp ladder (Bio-Rad Laboratories) as DNA molecular size standards. After PCR analysis the size of GBS amplification fragment was found to be 255 bp. Other streptococcal and staphylococcal species and Escherichia coli tested by scp B-gene-based PCR did not reveal any amplification bands. The internal control added to each PCR reaction allowed us to assess the efficiency of the amplification reaction and to ensure that PCR inhibition was absent. In addition, purified GBS DNA was used as a positive control. Multiple blanks were also included as negative controls to verify that there was no cross-contamination between samples. Statistical analysis Data were statistically described in terms of mean ± standard deviation (± SD), frequencies (number of cases), and relative frequencies (percentages) when appropriate. Comparison of quantitative variables between the two study groups was done using Mann Whitney U test for independent samples. For comparing categorical data, Chi square (χ2 ) test was performed. Yates correction equation was used instead when the expected frequency was < 5. A probability value ( P value) of < 0.05 was considered statistically significant. All statistical calculations were done using computer programs, Microsoft Excel version 7 (Microsoft Corporation, NY, USA) and SPSS (Statistical Package for the Social Science; SPSS Inc., Chicago, IL, USA). Results A total of 95 pregnant women were followed till delivery. Group A (GBS present) included 17 patients (17.89%) and group B (GBS absent) 78 patients (82.11%). The baseline characteristics and delivery data of both groups were similar [Table - 1]. Chorioamnionitis was not observed in any of the women by clinical criteria alone; whereas, three cases of chorioamnionitis were confirmed by placental pathology (one was in group A and two in group B) that was not statistically significant. Twenty two women had rupture of membranes (< 12 hours) before delivery (four from group A and eighteen from group B) and had undergone more than eight vaginal examinations but had not received antibiotics, statistically insignificant between the groups. The neonatal features of both groups [Table - 2] were also similar. As regards neonatal infection, there were three infants out of 17 in group A who were colonized (at one or more sites) by GBS against none out of 78 in group B which was statistically significant. However, only one infant was admitted to the neonatal intensive care unit (NICU) which was not statistically significant. Discussion During the past two decades, GBS or Streptococcus agalactiae has emerged as an important cause of perinatal morbidity and mortality. [7] In the present study, the prevalence of GBS colonization as detected by PCR was 17.89% and it was concordant with other reported rates of maternal GBS carriage. Patients with prolonged rupture of membrane (>12 hours) who received antibiotics were not included in the study, to avoid the theoretical effect on the PCR results of the neonatal samples. Using culture method, the carriage rate of GBS in Oxfordshire and London [18] is 21.3% but it is considerably higher in North Wales. This may be due to variant methodologies or may suggest geographical variations in GBS carriage within the United Kingdom. In Quιbec, GBS was detected in 33% of pregnant women by culture and in 32% by PCR, and the results were discordant only in one woman. Accurate PCR diagnosis requires selection of species-specific pairs of primers. The species-specific regions of 16S rRNA gene and 16S-23S intergenic spacer are often used for identification of bacteria and diagnosis of infections by PCR. Nevertheless, high homology of ribosomal operons in different species can end up with false-positive results. For example, this method caused the misidentification of S. agalactiae and S. difficile as the same species. [19] In our opinion, some other species-specific regions, for example, virulence genes, could be better candidate PCR targets. In the present study, the virulence gene scab encoding C5a peptidase was chosen as such a target. Previously, C5a peptidase genes were found only in GBS ( scp B gene), group A Streptococci ( scp A gene), and group G Streptococci ( scp G gene). Scp B gene being extremely homologous to scp A and scp G genes has a 51 bp deletion at the 3′-end of the gene. 1 In our study, this deletion was considered as GBS specific diagnostic marker. The increased sensitivity of our PCR assay may allow us to understand better the dynamics of vaginorectal GBS carriage in pregnant women. Colonization thought to be intermittent or transient [20] might rather be continuous, with variations in the bacterial load. Consequently, the predictive value of an antenatal GBS detection assay could increase significantly and be a better indicator of colonization at the time of delivery. This would be an important hypothesis to address in a future study. In the present study, the low incidence of documented early onset GBS disease and early onset sepsis, in general, were as expected. Neonatal infection was observed in three out of 17 neonates of the GBS colonized mothers against none from group B, which was statistically significant. However, this was not associated with any severe adverse fetal disease that required neonatal intensive care admission except in only one neonate and was statistically not significant. These results are limited by the small number of the population studied and calls for a wider multicenter study to address the geographical variations in Egypt and its reflection on neonatal morbidity and mortality. The data presented indicates that the scp B-gene-based PCR is a faster and more reliable test than microbiologic culture and can be considered as a very useful approach for the accurate diagnosis of infection. Suppression of growth of GBS by enterococci present in the vaginal and rectal flora was not evaluated in our study. However, we believe that PCR assays should not be adopted as a standard practice before quantitative GBS carriage in vaginorectal samples demonstrates whether a threshold predictive of neonatal disease exists. Without such studies, the increase in sensitivity would result in a much larger number of women receiving IAP without significantly diminishing the number of infants with neonatal GBS disease. In conclusion, maternal GBS carriage is associated with a significant increase in neonatal infection rate but is not associated with an increase in neonatal intensive care admission. An accurate evaluation of the colonization rate (using larger sample) to evaluate neonatal invasive disease and to determine whether PCR is cost effective is required for the selection of appropriate preventive strategies in Egypt. Future work in Egypt should focus on larger multicentric studies of GBS carriage in pregnant women, evaluation of culture versus rapid detection methods, and randomized controlled trials of strategies for prevention of neonatal GBS infection. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09004t2.jpg] [mb09004t1.jpg] |
| |||||||||
{kind=link}
{kind=link}