 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
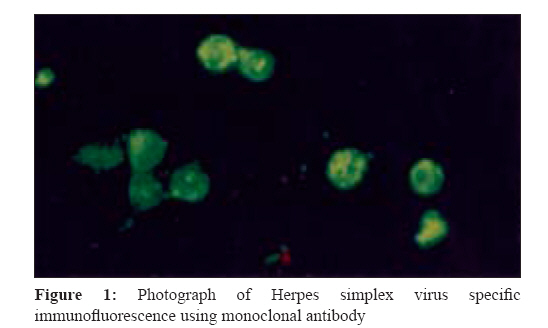
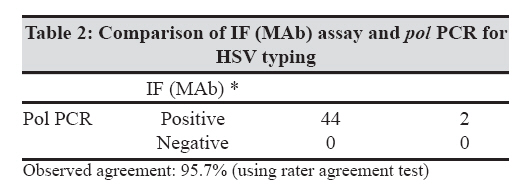
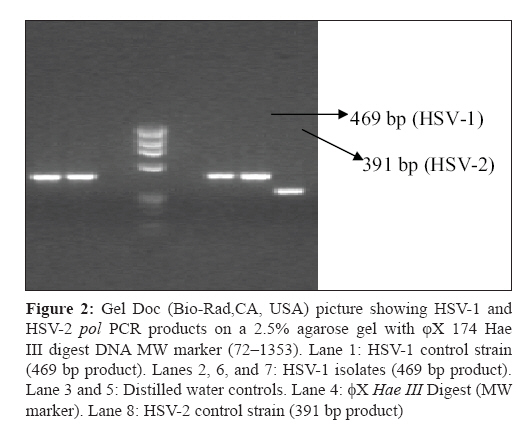
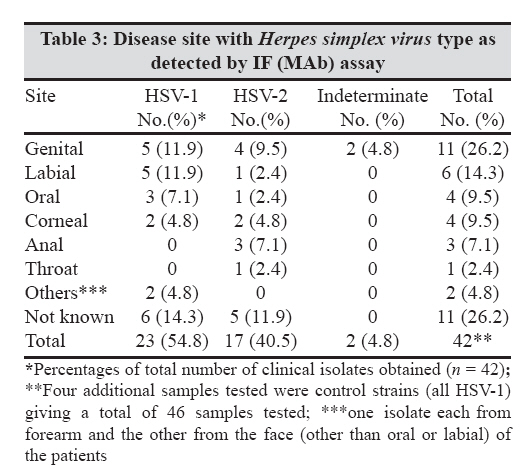
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 22-26 Original Article A molecular method for typing Herpes simplex virus isolates as an alternative to immunofluorescence methods Abraham AM, Babu M, Kavitha S, Jesudason MV, Sridharan G Department of Clinical Virology, Christian Medical College, Vellore - 632 004, Tamil Nadu Date of Submission: 16-Apr-2008 Code Number: mb09005 Abstract Background: Typing of Herpes simplex virus (HSV) isolates is required to identify the virus isolated in culture. The methods available for this include antigen detection by immunofluorescence (IF) assays and polymerase chain reaction (PCR). This study was undertaken to standardize a molecular method for typing of HSV and compare it with a commercial IF reagent for typing.Objectives: To compare a molecular method for typing HSV isolates with a monoclonal antibody (MAb) based IF test. Study design : This cross-sectional study utilized four reference strains and 42 HSV isolates obtained from patients between September 1998 and September 2004. These were subjected to testing using an MAb-based IF test and a PCR that detects the polymerase ( pol ) gene of HSV isolates. Results: The observed agreement of the MAb IF assay with the pol PCR was 95.7%. Fifty four point eight percent (23/42) of isolates tested by IF typing were found to be HSV-1, 40.5% (17/42) were HSV-2, and two (4.8%) were untypable using the MAb IF assay. The two untypable isolates were found to be HSV-2 using the pol PCR. In addition, the cost per PCR test for typing is estimated to be around Rs 1,300 (USD 30), whereas the cost per MAb IF test is about Rs 1,500 (USD 35) including all overheads (reagents, instruments, personnel time, and consumables). Conclusion: The pol PCR is a cheaper and more easily reproducible method for typing HSV isolates as compared to the IF test. It could replace the IF-based method for routine typing of HSV isolates as availability of PCR machines (thermal cyclers) is now more widespread than fluorescence microscopes in a country like India. Keywords: Hot start PCR, Herpes simplex virus, immunofluorescence, polymerase chain reaction, reagents, typing Introduction The spectrum of infections caused by Herpes simplex virus-1 (HSV-1) and Herpes simplex virus-2 (HSV-2) includes oropharyngeal, genital, and ocular lesions, neonatal infections, central nervous system infection, and multisystem infections in the immunocompromised. [1] The laboratory methods available for the diagnosis of HSV infections include isolation of virus, antigen detection, and molecular methods for direct demonstration of the virus as well as serological methods for diagnosing previous infection. [2] The most commonly used direct method of diagnosis is culture of HSV (from oral and genital swabs and ocular samples) in sensitive cell culture monolayers such as A549 and Vero cells. [3] Definitive identification can subsequently be carried out using immunofluorescence (IF), immunoperoxidase enzyme immunoassay, or radioimmunoassay methods. Most clinical virology laboratories use the IF technique for identification. [4] Although comparatively rapid, these methods require facilities for cell culture and a fluorescence microscope for IF. Reagents are also needed, their availability being variable in a developing country. Currently, the increasingly used molecular method is the polymerase chain reaction (PCR) which is very sensitive. [5] Also, today in countries like India, PCR machines (thermal cyclers) are more widely available than fluorescence microscopes in most diagnostic virology laboratories. Since the routine typing of HSV in the laboratory requires the use of expensive IF reagents that are not easily available in the market, we found it necessary to standardize a molecular method for typing of HSV and compare this method with a commercial IF reagent for typing. Materials and Methods This study was carried out at the Department of Clinical Virology in a tertiary care hospital in South India between September 1998 and September 2004. In the course of the study, 42 isolates were obtained from patients with HSV infection at various sites. The swabs collected from infected sites or the corneal scrapings were transported in viral transport medium placed in cold containers. Standard strains were obtained from Johns Hopkins Hospital (JHH), Baltimore, USA, and Health Protection Agency (HPA), Colindale, London, to verify the assays used in the study as previously reported. [6] Four standard strains were used and all the 46 isolates were confirmed to be HSV using anti-HSV polyclonal antibody tagged with FITC (Dako A/S, Denmark) following the manufacturer′s instructions. These 46 isolates were typed using monoclonal antibody (MAb) (Imagen Herpes simplex virus direct IF test, DakoCytomation, UK) according to the manufacturer′s instructions. Briefly for each isolate, when 70% of the infected Vero cell culture monolayer showed cytopathic effect, the cells were scraped into the liquid culture medium using a sterile pipette. The cells were centrifuged at 2000 rpm for 10 minutes at room temperature. The supernatant was then decanted and the cell deposit resuspended in 1x PBS pH 7.4 with a second centrifugation step as before. The cell deposit was resuspended in a small volume of fresh 1x PBS pH 7.4. Twenty-five microliters of cell suspension was placed onto each of the two wells on a microscope slide. The spots were air dried at room temperature, then fixed in fresh acetone for 10 minutes at room temperature. The slides were either stained immediately or stored at 4 °C overnight or at -20 °C if longer storage was needed. For staining, 25 µL of each monoclonal HSV reagent (one reagent per spot) was placed on each cell spot and incubated at 37 °C for 30 minutes in a moist chamber to ensure that the reagent did not dry on the specimen. The excess reagent was washed off with 1x PBS pH 7.4. The slides were washed gently in PBS in a slide washing bath for 5 minutes, drained, and allowed to air dry at room temperature. One drop of Imagen mounting fluid was added to the center of each spot and a cover slip placed over each spot carefully avoiding air bubbles. The slides of the infected cells were examined using a Leitz epifluorescence microscope (250X). Each run had positive and negative control spots which had to give the requisite fluorescence for a run to be considered valid. A sample was scored positive when the sample had three or more typically fluorescing cells per high power field (250X) [Figure - 1]. A PCR-based on the pol gene was performed as described previously using a common upstream primer HSV and specific downstream primers HSV-1 and HSV-2 [Table - 1]. [7] Standard recommended precautions were observed. [8] This test was used to determine the HSV type of each isolate as an alternative to the MAb IF test described as above. The DNA of each isolate was extracted using the QIAamp DNA Mini kit (QIAGEN GmbH, Germany) following the manufacturer′s instructions. The DNA was either used immediately for PCR or stored at -20 °C for long-term storage (used within six months). The primers used were as described previously. [7] The composition of the reaction mixture used was as follows: 10x PCR buffer 10 µL, 1 µL of 50 pM of each primer, 2.5 units Taq polymerase, 2 µL each dNTP, and 10 µL of the extracted DNA in a reaction volume of 100 µL. The reagents were obtained from Boehringer Mannheim (GmbH, Germany) and GeneCraft (Munster, Germany). The cycling conditions used were as described previously. [8] During the course of the study, it was found that the above reagents gave variable results (with samples giving variable results in consecutive runs), and hence, a hot start PCR reaction mix was standardized. The same primers described above were obtained from Invitrogen, Life Technologies (Carlsbad, CA, USA), and the composition of the hot start mix used was as follows: hot start Taq master mix 25 µL, 1 µL of each primer at 10 pM each, and 5 µL of extracted DNA made up to a final volume of 50 µL. The hot start PCR conditions used were: one cycle of 96 °C for 15 minutes followed by 35 cycles of 96 °C for 45 seconds, 58 °C for 40 seconds, and 72 °C for 35 seconds. A final extension of one cycle at 72 °C for 5 minutes completed each run. After thermal cycling, the products were analyzed using 1.5% agarose gel containing ethidium bromide. All 46 isolates tested by the MAb IF were tested by pol PCR as an alternate method of typing. Results Of the 46 isolates tested by IF assay, 42 were isolated from patients whereas four were standard strains. The results of the MAb based IF test performed on the 46 isolates were as follows: twenty eight of 46 (60.9%) were HSV-1, 16 of 46 (34.8%) were HSV-2, and two isolates (4.3%) were untypable. Using pol PCR as an alternate method of typing, the two strains that were untypable by IF were found to be HSV-2 as shown in [Table - 2]. The observed agreement of the IF assay with the pol PCR was 95.7%. [Figure - 2] is a gel picture demonstrating the specific pol PCR products generated for HSV-1 (469 bp) and HSV-2 (391 bp). The sites from which the 42 clinical isolates were obtained are given in [Table - 3]. Discussion In this study, 54.8% (23/42) of isolates tested by IF typing were found to be HSV-1, 40.5% (17/42) were HSV-2, and two (4.8%) were found to be untypable (excluding the four standard strains that were HSV-1 and the clinical sources of which are not known). In testing all the samples, particularly the two ′untypable′ isolates, it was ensured that the cell concentration was adequate and this was not a false-negative result. In contrast to this, another study did not show any indeterminate results using IF reagents from another commercial source. [9] The IF method also has the disadvantage of the need for expensive fluorescence microscopes, whereas thermal cyclers are more widely available in diagnostic laboratories in developing countries like India. Traditionally, typing of HSV is performed by IF using MAbs. At the beginning of this study, it was relatively easy to obtain the MAb IF reagents, but subsequently, the reagents were not available and another method had to be performed to type the HSV isolates. All isolates that were tested by pol PCR were typable by this method including the two that were untypable by IF. Hence, typing using the pol PCR method is found to be an optimal method for use in our country since the reagents are easily available and the shelf life for these reagents is longer than that for IF reagents. Another study from South India reported the use of PCR-based restriction fragment length polymorphism (RFLP) as a reliable, cost-effective, and less laborious method for typing of HSV from patients and culture-negative specimens. [10] In this study, typing of two standard strains and 23 clinical isolates was performed using type-specific HSV polyclonal antisera, PCR using allele-specific primers, DNA sequencing, and PCR-based RFLP. The results of all tests were concordant and, in addition, the PCR-based RFLP assay was able to detect HSV-1 and HSV-2 in 20 culture-negative samples. In yet another study from South India, four of 21 intraocular fluids tested were positive using a uniplex PCR for the HSV DNA pol gene, whereas a semi nested PCR (for the glycoprotein G gene) picked up an additional three positive specimens. The authors were of the opinion that the semi nested PCR could be used directly on clinical specimens. [11] HSV typing by cell culture methods was compared to direct antigen detection for diagnosis and typing in a study conducted in the UK. Cell culture was 81% sensitive and 100% specific as compared to PCR, while HSV enzyme immunoassay was 65% sensitive and 99% specific as compared to PCR. The added advantage of PCR-based detection was its ability to provide typing information. [12] The pol PCR used for typing in this study amplifies a 469 bp locus of the HSV-1 pol gene and a 391 bp locus of the HSV-2 pol gene using one common upstream primer and two downstream primers, one of which is specific for HSV-1 and the other for HSV-2. Its use has been described for detecting HSV in cerebrospinal fluid along with DNA probe detection. [7] We found that the pol PCR as described did not amplify 10 TCID 50 /10 μL of input virus. For the purpose of detecting most strains of HSV in culture, however, it was found to be adequate. Subsequent culture of some resistant viruses required the use of hot start reagents as the results were found to be more reliable with these reagents and using the same set of primers. Routine DNA polymerases show a low level of template extension at room temperature. This is usually not a problem for routine PCR applications where the template is present above 100-500 copies. However, when the target template is below this level, this room temperature extension can pose a major problem. The basis of hot start PCR reactions is the use of proofreading enzymes that require elevated temperatures to be active. [13] The pol PCR method used in this study was estimated to cost about Rs 65,000 (USD 1,512) for 50 tests, while the cost of MAb IF assay was about Rs 75,000 (USD 1,744) for the same number of tests (per test costs working out to Rs 1,300 or USD 30 and Rs 1,500 or USD 35, respectively). These figures have been calculated for all overheads involved namely reagents, instruments, personnel time, as well as consumables. This is not surprising since primers are now indigenously manufactured and easily available, whereas MAb reagents are imported, and hence, comparatively more expensive. The disease sites associated with the HSV types as shown in [Table - 3] highlight an important change in the epidemiology of HSV-related infections. The two isolates that were not typable by MAb IF assay were typed as HSV-2 by pol PCR. Thus, 54.5% (6/11) of the genital isolates were actually HSV-2 as compared to 45.5% (5/11) that were found to be HSV-1 by PCR. These numbers are too small to be used to project an epidemiological pattern. A previous study in our hospital [9] demonstrated that 85% of genital herpes was caused by HSV-2. More recently, there has been a marked change observed in the proportion of HSV-2 to HSV-1 in the etiology of genital herpes (GH) infection in some populations. [14] In this study, it was found that the proportion of newly diagnosed GH infection due to HSV-1 rose from 31% to more than 78% between 1993 and 2001 among a population of college students. This change was attributed to orogenital contact with an infected partner. Changing sexual practices in our population too could be reflected in the increase in HSV-1 etiology of GH. It would, however, require further epidemiological studies to confirm this finding in our population. Most of the other disease sites in our study show the ′expected′ distribution of HSV type (HSV-1 in labial, oral and facial, and arm skin sites while HSV-2 was isolated from anal sites of patients). The pattern of HSV-2 in etiology of ocular samples been described previously. [15],[16] Again, a thorough epidemiological study is needed to elucidate the role of HSV-2 ocular infections in Vellore. Conclusions The pol PCR method used in this study to determine the HSV type is an easily reproducible method for typing HSV as compared to the monoclonal antibody based IF. Moreover, the reagents are more easily available, have a longer shelf life, and are cheaper than those for IF. In developing countries, laboratories that have PCR facilities will find the pol PCR to be a relatively simple technique to perform and one that does not require the capital involved in obtaining a fluorescence microscopes. The pol PCR could be used to type all isolates of HSV in routine clinical virology laboratory practice.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09005t2.jpg] [mb09005t3.jpg] [mb09005t1.jpg] [mb09005f2.jpg] [mb09005f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}