 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
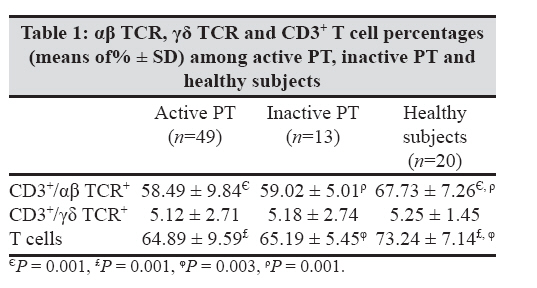
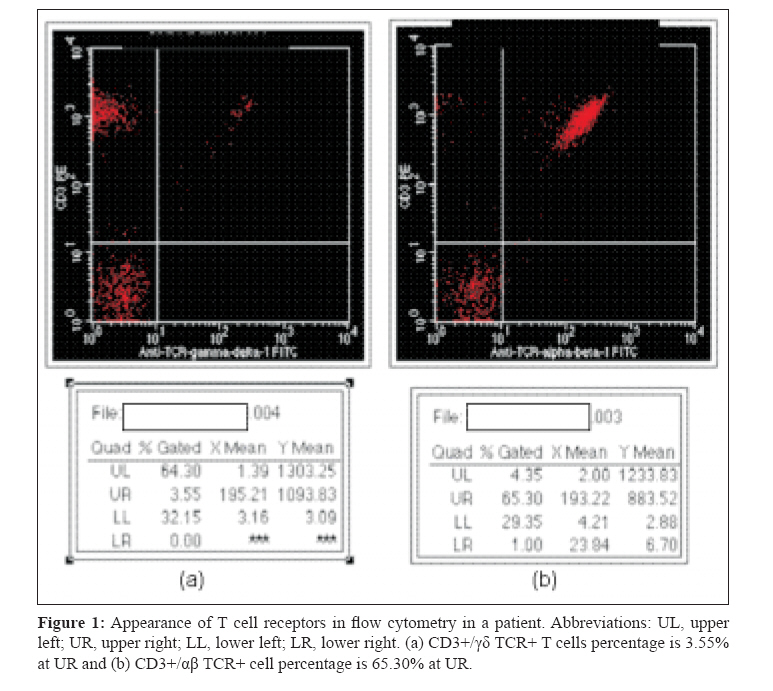
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 40-43 Brief Communication Investigation of T cell receptors in the peripheral blood of patients with active pulmonary tuberculosis Akbulut HH, Deveci F, Celik I, Ilhan F, Turgut T Department of Immunology, Faculty of Medicine, Firat University, Elazig 23119 Date of Submission: 09-Oct-2007 Code Number: mb09009 Abstract T cells have the capability of recognizing target cells through their T cell receptors (TCRs). Thus, the percentages of CD3 +/ gamma-delta (γδ) TCR+ and CD3 +/ alpha-beta (αβ) TCR+ T lymphocytes were investigated in active and inactive pulmonary tuberculosis (PT) patients and in healthy individuals. CD3 + and CD3 +/αβ TCR+ cell percentages were significantly lower in all PT patients than in healthy subjects. Percentages of CD3 +/γδ and CD3+/αβ TCR+ were not statistically different between active and inactive PT patients. It was concluded that αβ TCR+ T cells might have a protective role in tuberculosis infection.Keywords: Alpha/beta T cell, gamma/delta T cell, tuberculosis Mycobacterium tuberculosis is a major cause of morbidity and mortality worldwide. After M. tuberculosis infection by inhaling aerosolized bacteria, the majority of infected individuals develop a cellular immune response and arrest growth and spread of the microorganism without progressing to clinical tuberculosis. [1] Cellular immune responses are a critical part of the host′s defense against intracellular bacterial infections. [2] T cells have the capability of recognizing target cells through their T cell receptors (TCRs). Progress has been made about the nature and regulation of antigen-specific γδ T cell responses in mycobacterial infections. [3] As T cells express ab receptors that elucidate T-helper function and cytotoxic activity, gd T cells have a potent cytotoxic effect. [4] Despite extensive research, the mechanisms of immune protection to tuberculosis are not completely understood. This study, aimed at comparing γ/δ and α/β receptors of the T cells at active and inactive periods of patients diagnosed with tuberculosis. Materials and Methods Patients and study design The study was performed on randomly selected 49 active pulmonary tuberculosis (PT) patients (mean±SD age, 35.76±15.8, 22 men and 27 women) who had been admitted to the Department of Chest Diseases of Firat Medical Center and Elazig Tuberculosis Dispensary. Pulmonary tuberculosis PT was diagnosed by the following parameters: presence of cough/expectoration, chest X-ray showing infiltrates and/or cavities, a minimum of one positive sputum smear and culture result for acid-fast bacilli. The extrapulmonary involvement was not established for any patients. The exclusion criteria were human immunodeficiency virus (HIV) positivity, diabetes mellitus, pregnancy and immunological or autoimmune diseases. Active PT patients were divided into three groups according to the treatment as follows: According to the antituberculosis treatment Group 1 was composed of 25 newly diagnosed active PT patients. None of these had prior tuberculosis history. Group 2 included 18 patients who had undergone 2-month antituberculous treatment with quartette drugs (rifampicin, pyrazinamide, isoniazid and streptomycin or ethambutol). Group 3 included six patients who had been treated with antituberculous drug for 6 months. [5] Thirteen inactive PT cases (mean±SD age 43.23±20.5, five women and eight men) that were registered and treated in the Elazig Tuberculosis Dispensary and 20 healthy volunteer subjects (mean±SD age 38.20±17.6, nine women and 11 men) were included as a control groups. Inactive PT patients had a history of previous episode of tuberculosis with documentation of a positive culture at the time of diagnosis. There were abnormal stable radiographic findings and no change in the last 6 months. Three sputum cultures for M. tuberculosis were negative in all patients. [6] Healthy subjects did not have any changes on X-ray and tuberculosis history or other underlying disease and they were not currently taking medication. Exclusion criteria for the healthy control groups were smoking, medication, pregnancy and any abnormalities in renal and liver function tests. Acid-fast bacilli stains were performed according to the Ziehl-Neelsen method. Cultures for M. tuberculosis were performed in the Lowenstein-Jensen medium. The tuberculin test was performed according to the Mantoux test - intradermal 5 Todd Unit PPD (BB-NCIPD Ltd., Sophia, Bulgaria) injected into the volar surface of the forearm and the results were evaluated 72 h later. The transverse induration of ≥ 10 mm was considered as a positive response. All active and inactive PT patients had a positive PPD skin test. Healthy control subjects had been vaccinated with BCG as part of the "Turkey National Vaccination Program" and thus all were tuberculin positive. The specialist filled the questionnaire forms by asking about symptoms of the disease. The Local Ethics Committee approved the study. All individuals gave informed consent. Flow cytometric analysis of peripheral blood Having performed these applications, 5 mL of venous blood from the individuals diagnosed as tuberculous and healthy subjects was drawn into the tubes with ethylenediaminetetraacetic acid in order to examine the TCRs by flow cytometry. All blood samples were researched within 2 h. Peripheral blood samples were analysed on the Coulter EPICS XL-MCL (Beckman Coulter, Fullerton, California, USA) by using the Immunotech (Marseille, France) monoclonal antibodies (mAb). Cell surface expression of lymphocyte antigens was examined by mAb staining of peripheral blood samples two-color flow cytometry. CD14/CD45, isotype control, CD3/TCRαβ, CD3/TCRγδ mAb tubes were prepared and analysed according to the instructions of manufacturer. A total of 10.000 cells were counted, and the results were interpreted using isotypic controls after performing the voltage tunings required. Results were counted at the same equipment using the Expo-32 analysis software (Beckman Coulter Company, Miami, Florida 33196-2500 USA). The lymphocyte population was expressed as percentages of the total number of lymphocytes. The quality criteria involved the frequency above 95% of the total lymphocytes in the analysis gate, and a homogenous CD45 + lymphocyte population (minimum of 2000 events in the gate, CD45>95%). Statistical analysis The data were expressed as their arithmetic means with standard deviations. The MannWhitney U -test and Spearman′s correlation analysis were performed by using the SPSS 12.0 packet software (SPSS Inc., Chicago, Illinois 60606-6307, USA). Statistical significance was interfered at a P -value < 0.05. Results There were no statistically significant differences according to the age or gender among the groups. The mean PPD response was statistically higher in active PT (15.35 ± 2.78, range 11-24 mm) and inactive PT (13.92 ± 2.25, range 10-17 mm) than in healthy subjects (11.80 ± 1.64, range 10-16 mm) ( P = 0.000 for active PT and P = 0.007 for inactive PT compared with healthy subjects). There were no correlations between PPD and TCRs and T lymphocyte counts in active or inactive PT patients or healthy subjects ( P > 0.05 for all groups). The percentages of (means of% ± SD) gd TCR, αβ TCR and T lymphocyte counts are given in [Table - 1]. [Table - 1]: αβ TCR, γδ TCR,and CD3+ T cell percentages (means of% ± SD) among active PT, inactive PT and healthy subjects Patients with active and inactive PT had lower T cell counts than healthy subjects ( P = 0.001 and 0.003 respectively). There was no statistically significant difference between the groups concerning T cells bearing gd TCR. Patients with active PT and inactive PT was lower in the groups with regard to T cells bearing αβ TCR than in healthy subjects ( P = 0.001). There were no statistical differences observed regarding γδ TCR and CD3+ T lymphocyte between all groups in active PT ( P > 0.05). CD3 + T lymphocyte and ab TCR + T cells were found lower in the first group of active PT than in healthy controls ( P = 0.004 and 0.001; P = 0.001 and 0.001 respectively). Also, CD3 + T lymphocyte and αβ TCR + T cells were found lower in the second group of active PT than in healthy controls ( P = 0.003, 0.001 and 0.006; P = 0.003 respectively). However, there were no statistically significant differences in γδ TCR+ T cells among the groups of patients with active PT. There were no statistically significant differences concerning these parameters when comparing the third group of patients with active PT with healthy subjects ( P > 0.05). No statistically significant differences were observed concerning these parameters when comparing groups of patients with active PT with patients with inactive PT ( P > 0.05). Images of TCR-bearing cells obtained from flow cytometry are shown in [Figure - 1]. [Figure - 1]: Appearance of TCRs in flow cytometry in a patient. Discussion The aim of this study was to evaluate the population of gd and ab T lymphocytes in the peripheral blood of patients with active and inactive PT in an attempt to offer insights into the role played by these cells in immunity against M. tuberculosis . ab receptor genes are expressed in a majority of peripheral T cells.. On the contrary, gd receptor genes are found as a part of thymocytes and a small part of peripheral T cells. In genetically modified animals without gd T cells, it is observed that resistance to infections is deficient. [7] Dramatically, proliferation of gd T cells was demonstrated in the bloods of cases infected by some bacteria such as M. tuberculosis, Franciella tularensis, L. monocytogenesis, L. donovani and Plasmodium falciparum. [4] A majority of γδ T cells bear on the same pair of TCR - Vγ9Vδ2 and share antigenic specificity. Therefore, they act in a rapid and potent manner in the early phase of immune response to a pathogen and cellular damage. [7] Recent studies have established that besides CD4 + αβ TCR+ cells, both CD8 + αβ TCR+ T cells and γδ TCR + T cells have a role in the cellular immune response to mycobacteria. On the contrary, it was found that no difference exists between active and inactive PT and healthy subjects in terms of γδ TCR+ T cells. [8] In the current study, percentages of CD3 + T lymphocytes and αβ TCR + T cells were found lower in the first group of patients with active PT than in healthy subjects ( P = 0.004 and 0.001 respectively). Ladel et al . [9] showed in an experimental study that mice lacking γδ T and αβ T cells suffer a more severe form of tuberculosis and fail to control the infection. They found that the crucial role of αβ T cells is protection against established tuberculosis and formally proved a protective role of γδ T cells in early tuberculosis. Our results are similar to Ladel et al′s as we confirm the crucial role of αβ T cells in protection against established tuberculosis. On the contrary, we did not observe any statistical differences concerning γδ T cells between the different groups of active PT and those taking different treatments and healthy subjects. Like our study, Li et al . [10] reported that the γδ T cell subset distribution is altered in some M. tuberculosis -infected patients. In a study performed by Szereday et al ., [11] the γδ T cell distribution is particularly affected in tuberculin-negative patients (γδ T cells were significantly higher in patients with a negative tuberculin reaction than in a tuberculin-positive healthy control). Similarly, Carvalho et al . [12] found that HIV-seronegative tuberculosis patients had lower total lymphocyte and CD4 + T proportions than healthy blood donors but a similar total δγ T cell and V1δ1 subset proportions. In addition, Baliko et al . [13] reported that no difference is found in the percentage of γ/δ T lymphocytes between patients and controls, and in addition a higher percentage of γ/δ T lymphocytes are found in the peripheral blood of patients with tuberculin anergy than in tuberculin-positive patients or controls. In this study, it was observed that the γδ T cell distribution was not affected in tuberculin-positive patients and that αβ TCR+ T cells were found lower in patients than in healthy subjects. It was concluded that αβ TCR+ T cells might have a protective role for tuberculosis infection. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09009f1.jpg] [mb09009t1.jpg] |
| |||||||||
{kind=link}
{kind=link}