 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
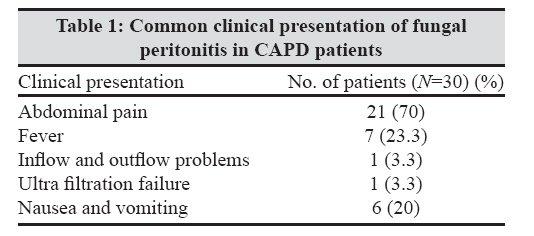
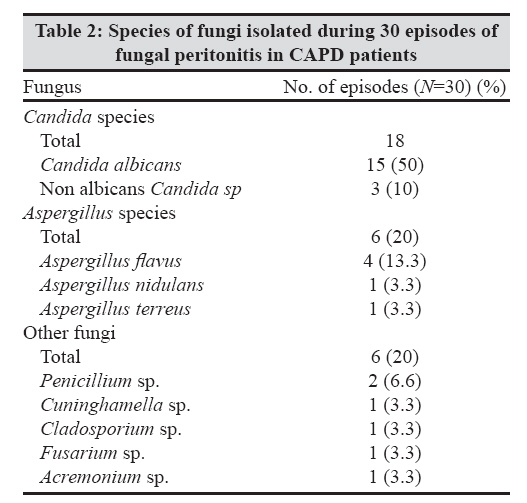
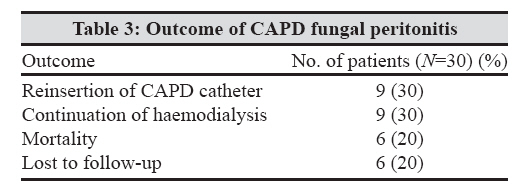
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 59-61 Brief Communication The risk factors and outcome of fungal peritonitis in continuous ambulatory peritoneal dialysis patients Indhumathi E, Chandrasekaran V, Jagadeswaran D, Varadarajan M, Abraham G, Soundararajan P Department of Nephrology, Sri Ramachandra University, No. 1, Ramachandra Nagar, Porur, Chennai-600 116, Tamil Nadu Date of Submission: 20-Feb-2008 Code Number: mb09014 Abstract Aim: To determine the risk factors and outcome of fungal peritonitis in continuous ambulatory peritoneal dialysis (CAPD) patients over a 7-year period.Patients and Methods: This retrospective study was conducted on 30 cases of fungal peritonitis in CAPD patients during a 7-year period (2000-2007). The diagnosis was based on elevated CAPD effluent count and isolation of fungi. Patients were evaluated for previous episode of bacterial peritonitis. Results: The incidence of fungal peritonitis was 16.2%. Age varied between 8 and 75 years, with a mean age of 57 years. Twenty-three were males (76.7%) and seven were females (23.3%). Seventeen patients (56.6%) had previous episodes of bacterial peritonitis that was treated with multiple antibiotics. The common fungus was Candida species (50%). CAPD catheter removal and initiation of antifungal therapy was done for all patients. Reinsertion was done for three (10%) patients. Mortality rate was 20%. Conclusion: Patients with previous bacterial peritonitis and antibiotic usage are at greater risk of developing fungal peritonitis. Keywords: Antifungal therapy and catheter removal, continuous ambulatory peritoneal dialysis, fungal peritonitis, prior antibiotic usage Continuous ambulatory peritoneal dialysis (CAPD) is an increasingly popular replacement therapy in end-stage renal disease. However, peritonitis continues to be a frequent complication of CAPD. Pathogenic bacteria and a small number of fungi cause the majority of cases of peritonitis. Nevertheless, fungal peritonitis remains a serious complication associated with high rates of morbidity and mortality. [1] Mortality rate is variable, with as high as 50% with fungal peritonitis Forty per cent of patients with an episode of fungal peritonitis are switched over to haemodialysis. [2],[3],[4] The most common cause of fungal peritonitis is Candida species, with Candida albicans predominating. [2],[4] Fungi enter the peritoneal cavity through touch contamination of dialysis tubing or by direct extension of the infection from the catheter exit site. [5] Clinically, fungal peritonitis cannot be differentiated from bacterial peritonitis except by Gram stain and culture of dialysate effluent. [6] The treatment of fungal peritonitis is difficult and needs, in majority of the cases, the CAPD catheter removal because the fungi form a biofilm on the surface of the catheter, which reduces the penetration of antifungal agents. In this study, the incidence, the risk factors involved and the outcome of fungal peritonitis were evaluated in 185 CAPD patients during the period of 2000-2007. Patients and Methods This retrospective study was conducted on 30 cases of fungal peritonitis among 185 CAPD patients during a 7-year period (2000-2007) in our centre. CAPD was performed manually in all these patients. Patients were evaluated for previous episode of peritonitis, clinical manifestations such as abdominal pain, vomiting, fever, abdominal tenderness, cloudy dialysis effluent, exit site infection and ultra filtration failure. The diagnostic criteria for fungal peritonitis included CAPD effluent cell count of 100 or more WBCs per microlitre, differential count of more than 50% polymorphonuclear cells and isolation of the fungus. Patients with a negative fungal culture were excluded. The specimen sent for fungal peritonitis included CAPD fluid and CAPD catheter. Distal 2.5-5 cm of the CAPD catheter was cut from the catheter hub and dropped into a sterile container. The CAPD fluid was centrifuged at 10,000 rpm for 5 min. The sediment was used for microscopic examination with 10% KOH to look for fungal elements. The CAPD catheter tip was flushed with sterile saline using a needle and syringe and this was used for microscopy as above. The fluids from the above procedure were inoculated into the following media in duplicates: (a) Sabouraud′s dextrose agar with gentamicin and (b) Potato dextrose agar. One set of tubes were incubated at 37°C and the other set was incubated at 25°C. The cultures were examined every 2 days for a period of 1 month for the presence of growth. If no growth was found after 1 month, it was considered negative for the growth of fungi. Growth obtained was identified based on macroscopic and microscopic morphology. The identification of the growth was based on the growth rate, temperature requirement and colony characteristics on the obverse, like colour, texture, pigment and submerged hyphae. The colony characteristics on the reverse were also studied for the presence or absence of pigment and whether diffuse or localized. After observing the colony morphology, moulds and yeasts were identified according to the standard procedures. Results The incidence of fungal peritonitis was 16.2% with 30 patients among 185 CAPD patients developing fungal peritonitis. Age ranged from 8 to 75 years, with a mean age of 57 years. Twenty-three were male and seven were female. The mean duration of CAPD before development of fungal peritonitis was 17.29 months (range 3-48). The primary renal disease leading to end-stage renal disease was diabetic nephropathy in 18 patients, chronic glomerulonephritis in nine patients and hypertensive nephropathy and obstructive nephropathy in each patient. In one patient, the exact etiology of the primary renal disease was not clear. Among the patients who developed fungal peritonitis, 17 patients (56.8%) had one or more previous episode of bacterial peritonitis that was treated with multiple broad-spectrum antibiotics. Six (20%) of them had more than two episodes of bacterial peritonitis. Three (10%) had two episodes and eight (26.6%) had one episode of bacterial peritonitis. Bacteria included Streptococcus sp, Corynebacterium sp, Staphylococcus aureus and Pseudomonas sp. The common clinical presentation [Table - 1] was abdominal pain and fever. Others included were inflow and outflow problems, ultra filtration failure and vomiting. Fungal stain was positive in 21 (70%) patients. The commonest fungus isolated [Table - 2] was Candida albicans in 15 patients (50%) while the others were non albicans Candida sp, Aspergillus flavus , A. nidulans , A. terreus , Penicillium sp, Cuninghamella sp, Acremonium sp, Cladosporium sp and Fusarium sp. CAPD catheter was removed in all patients at the time of diagnosis of fungal peritonitis and they were treated with antifungal therapy. Patients were temporarily initiated on haemodialysis. Reinsertion was done for nine patients (30%) 4 weeks after the episode of fungal peritonitis. Nine patients (30%) were continued on haemodialysis as they were not willing for catheter reinsertion and continuation of CAPD. Six patients (20%) died during the episode of fungal peritonitis. Four patients were lost to follow-up. Discussion Although fungal peritonitis is uncommon in patients undergoing CAPD, it accounts for serious morbidity and mortality. [1] In most series 2-10% of CAPD-related peritonitis episodes have a fungal aetiology, of which 80-90% were Candida species and less frequently by other species. [7] Fungi enter the peritoneal cavity through touch contamination of dialysis tubing or by direct extension of the infection from the catheter exit site. [5] Antimicrobial therapy causes alteration of faecal flora and transmigration of organisms into the peritoneal cavity. The fungus colonizes the peritoneal catheter and is embedded in the amorphous matrix on the surface of the catheter leading to fungal peritonitis. In our study population, age, gender, underlying aetiology, comorbid disease and duration of dialysis did not have any significant association with the development of fungal peritonitis. Seventeen patients (56.8%) in our study had one or more previous episodes of bacterial peritonitis and received antibiotics. This agrees with another study by Prasad et al . [8] in which the preceding bacterial peritonitis as a risk factor was 25.6 %. Goldie et al. and Stanley et al . [8],[9],[10] showed that the previous antibiotic therapy was the main predisposing clinical condition for fungal peritonitis. The commonest fungus isolated was Candida species, which accounted for 60% of our patients. Johnson et al . [5] found that 90% of the cases of fungal peritonitis were caused by Candida species. Other studies by Manzano-Gauossa et al . and Bren [10],[11],[12] also found that Candida was the predominant fungus isolated from CAPD patients with fungal peritonitis. CAPD catheter was removed in all patients at the time of diagnosis of fungal peritonitis and they were initiated on antifungal therapy. There is no unified strategy for treatment of fungal peritonitis. Nagappan et al . [2] managed most of their cases first by early catheter removal. Antifungal therapy was initiated in those cases where symptoms and signs did not improve within 48 h after catheter removal or seriously ill patients. In our study, 20% of the fungal peritonitis patients died. Mortality rate is variable and could be as high as 53.6%, particularly if catheter removal is delayed by more than 24 h. Chan et al . [3] had a mortality of 14.3% in their study population. Reinsertion and initiation of dialysis could be done successfully for 10 (30%) of our patients 2-8 weeks later. Others were continued on haemodialysis or were lost to follow-up as shown in [Table - 3]. Conclusion Patients with previous bacterial peritonitis and antibiotic usage are at greater risk of developing fungal peritonitis. Antifungal therapy and early catheter removal will reduce the mortality rate of CAPD fungal peritonitis.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09014t3.jpg] [mb09014t1.jpg] [mb09014t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}