 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
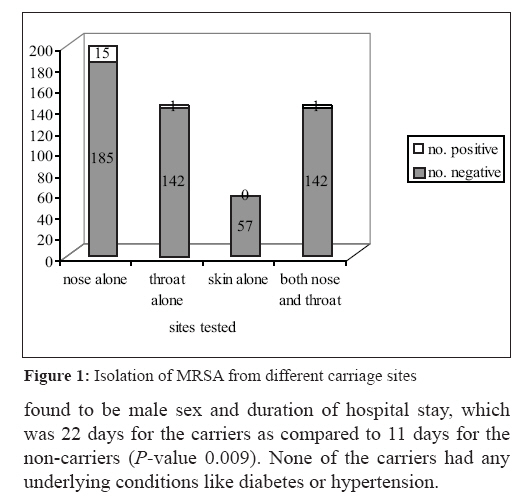
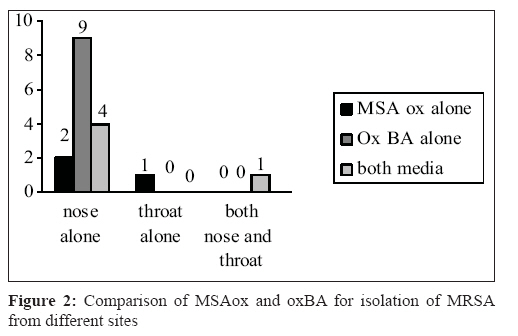
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 62-64 Brief Communication Screening for methicillin-resistant Staphylococcus aureus carriers among patients and health care workers of a tertiary care hospital in south India Mathanraj S, Sujatha S, Sivasangeetha K, Parija SC Department of Microbiology, Jawaharlal Institute of Postgraduate Medical Education and Research, Pondicherry 605 006 Date of Submission: 21-Feb-2008 Code Number: mb09015 Abstract A total of 200 subjects were screened for carriage of methicillin-resistant Staphylococcus aureus (MRSA) at different sites using oxacillin blood agar and mannitol salt agar with oxacillin. Overall carriage rate was 8.5%, with the highest rate in inpatients (15.6%) while the lowest was seen in health care workers (1.8%). The commonest site of colonization was the anterior nares. Oxacillin blood agar was found to be superior to mannitol salt agar with oxacillin for the isolation of MRSA. Male sex and prolonged hospital stay were found to be the major risk factors for MRSA colonization.Keywords: Health care workers, methicillin-resistant Staphylococcus aureus carriage, patients, risk factors, selective media Asymptomatically colonized patients and health care workers are the major sources of methicillin-resistant Staphylococcus aureus (MRSA) in the hospital environment, with the latter being more commonly identified as links in the transmission of MRSA between patients. [1] Screening for MRSA carriers among this population is necessary for nosocomial infection control. Several selective media have been used for this purpose, such as mannitol salt agar with oxacillin and CHROM agar, with varying rates of success. [2],[3] The objectives of the present study were to screen patients and health care workers for MRSA carriage, to evaluate two selective media (mannitol salt agar with oxacillin and oxacillin blood agar) for their efficiency in isolating MRSA from various specimens and to identify risk factors for MRSA colonization. Methods A total of 200 subjects (90 inpatients, 53 outpatients and 57 health care workers) were screened for MRSA after obtaining informed consent and approval by the institute ethics committee. Clinical details including duration of hospital stay, diagnosis, antibiotic intake and presence of other medical illnesses were recorded for the inpatients. The outpatients were included after ascertaining that they had not visited a hospital in the previous 1 year and had no contact with any health care worker. Using pre-moistened sterile cotton swabs, specimens were collected from the anterior nares and throat of patients and the anterior nares, palms and web spaces of health care workers. The specimens were inoculated onto oxacillin blood agar and mannitol salt agar with oxacillin and incubated at 37 0 C in ambient air for 24-48 h. Colonies suggestive of S. aureus (white or cream haemolytic or non-haemolytic colonies on oxacillin blood agar and yellow colonies on mannitol salt agar) were identified using Gram stain, catalase and slide and tube coagulase tests. The isolates were confirmed as MRSA both by disc diffusion (1ug oxacillin) and agar dilution methods. Statistical analysis of the risk factor association with MRSA colonization was calculated using the Chi-square test (Epi info software). Results A total of 17 strains of MRSA were isolated from 200 subjects, giving an overall positivity rate of 8.5%. Fourteen of them were from inpatients (14/90, 15.6%), two from outpatients (2/53, 3.8%) and one from a health care worker (1/57, 1.8%). A majority of the carriers were males (15/118, 12.4% vs 2/82, 2.4%).This difference in the sexes was found to be statistically significant, with a P -value < 0.01, an odds ratio of 5.83 (95% CI, 1.2-38.02). Inpatients in orthopaedic surgery, general surgery and dermatology wards accounted for most of the carriers (12/14). Fifteen of the 17 carriers (88.2%) were found to be colonized in the anterior nares alone, whereas only one of them was found to carry the organism in the throat [Figure - 1]. Oxacillin blood agar was found to be superior to mannitol salt agar with oxacillin for isolation of MRSA [Figure - 2]. Of the 17 isolates, 14 grew on oxacillin blood agar (82.3%) whereas only eight grew on the latter (47%). A total of nine strains grew only on oxacillin blood agar while three grew exclusively on mannitol salt agar with oxacillin. The significant risk factors for MRSA colonization were found to be male sex and duration of hospital stay, which was 22 days for the carriers as compared to 11 days for the non-carriers ( P- value 0.009). None of the carriers had any underlying conditions like diabetes or hypertension. Discussion The overall MRSA carriage rate of 8.5% in the present study with the highest rates seen among inpatients (15.6%) is consistent with other reports in the literature. Most studies had focused on patients belonging to particular wards like dermatology and burns units where the likelihood of colonization is high. [4],[5] MRSA-infected patients in burns units are particularly problematic because the big surface area of denuded skin can produce a large inoculum of organisms that can be easily transmitted to other patients via the hands of health care workers. The same is true of dermatology wards where extensive skin lesions also result in heavy shedders of MRSA. In the present study, the highest rate of carriage was among inpatients of the orthopedic and dermatology wards. The carriage rate among outpatients was low at 3.8%. Both the carriers were adult males without any antecedent contact with the health care environment at least in the previous year. Whether these strains constitute the true CA-MRSA or not needs to be studied. Earlier reports of these strains were mainly from children and young adults where they were shown to cause skin and soft tissue infections. [6],[7] Only one health care worker was found to be a nasal carrier of MRA in our study. This is in contrast to other studies where rates of 6-50% have been described in the health care workers, particularly those posted in the burns and in the intensive care units. [8],[9] Males were more likely to be MRSA carriers than females. Only one other study has found a marginally higher prevalence of MRSA carriage in males, although it was not statistically significant [10] The reasons for this male preponderance needs to be further studied, including the possible role of hormones. The commonest site of MRSA carriage in the present study was found to be the anterior nares, which is similar to many reports. In a study of 403 carriers, the sensitivities of different sampling sites were 78.5% for nose alone, 85.6% for nose and throat and 98% when perineum was included. [11] The sensitivity of nasal swab alone was found to be 94% in our study. Oxacillin blood agar was found to be superior to MSAox in the present study for isolating MRSA from various sites. This is in contrast to the reports of others where MSA was found to be the most efficient medium, particularly when lipovitellin was added to it. [2] The reason for this poor performance could be the high concentration of salt used in our study (10%). Some studies have shown that a few S. aureus strains may also be inhibited at this concentration. Another reason could be that mannitol may not be fermented by all strains, which would make them unrecognizable on this selective medium. [12] After the results of the study were obtained, we tested all the strains for their ability to ferment mannitol and found that six of the eight strains that did not grow on MSA were indeed mannitol negative. This very high percentage of mannitol-negative strains in our study precludes the use of this selective medium at least in our hospital in future. Moreover, another disadvantage with MSA was the delay in obtaining visible colonies (48 h vs 24 h on blood agar). The other significant risk factor for acquisition of MRSA found in our study was the duration of hospital stay, which is similar to other reports in the literature. [13] Prolonged stay in the hospital is likely with patients in orthopedics and dermatology wards, which would explain the high rates of carriage observed in these patients. Other major risk factors like previous antibiotic use and underlying illnesses were not commonly encountered in our patients. Health care workers do not appear to be a major source of MRSA in our hospital, although it would require screening of larger numbers before arriving at any definite conclusions. Regular screening of all inpatients may neither be feasible nor warranted, but selective screening in high-risk areas may prove beneficial. If performed, nasal screening alone is sufficient. Finally, it is recommended that local isolates of S. aureus be tested for mannitol fermentation before adopting mannitol salt agar as a selective medium. Acknowledgement This study was carried out as a short term project granted by the Indian Council of Medical Research to undergraduate students of medicine.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09015f2.jpg] [mb09015f1.jpg] |
| |||||||||

{kind=link}
{kind=link}