 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
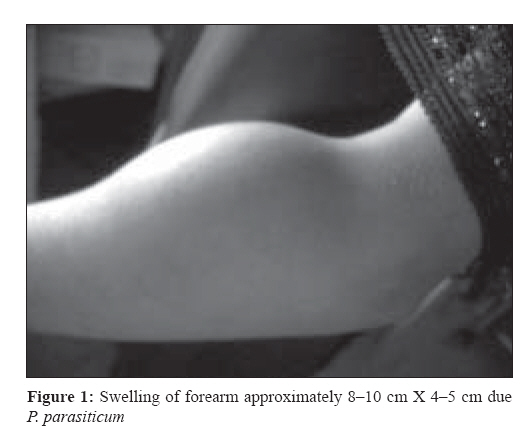
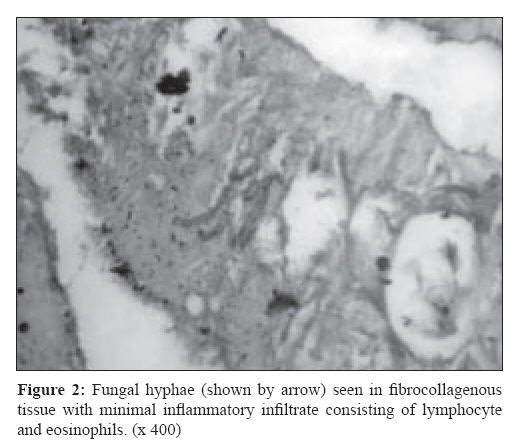
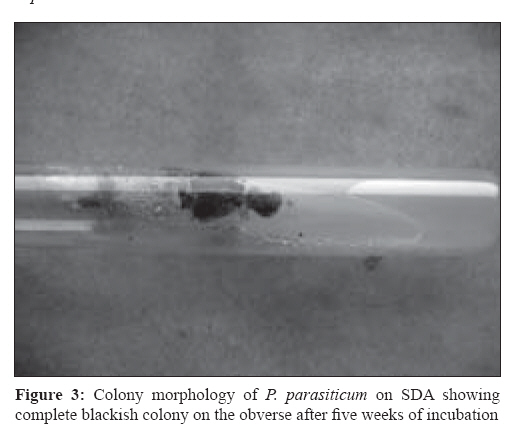
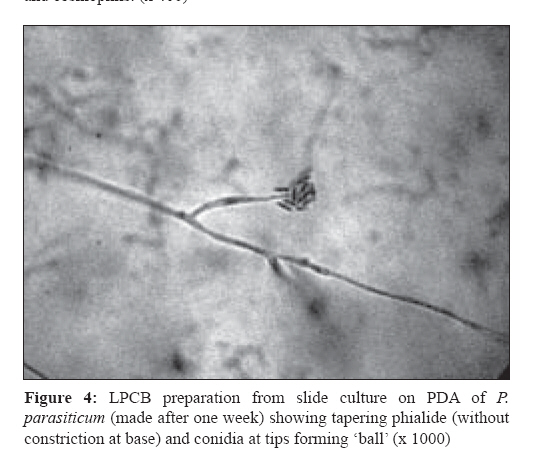
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 66-69 Case Report Phaeohyphomycosis of subcutaneous tissue caused by Phaeoacremonium parasiticum Baradkar VP, Mathur M, Kumar S Department of Microbiology, Lokmanya Tilak Municipal Medical College and General Hospital, Sion, Mumbai- 400 022 Date of Submission: 08-Jun-2008 Code Number: mb09017 Abstract Though Phaeoacremonium parasiticum is an unusual cause of human disease, subcutaneous infection, eumycetoma, osteomyelitis, arthritis and even disseminated diseases, such as fungemia and endocarditis have been reported. Here, we report a case of subcutaneous abscess on the forearm due to P. parasiticum in a 26-year-old woman. There were no obvious predisposing factors. The patient was treated with surgical debridement followed by intravenous amphotericin B and itraconazole to which she responded well. We report this case, being rare and the first from India.Keywords: Phaeoacremonium parasiticum, subcutaneous infection Human disease caused by Phaeoacremonium parasiticum is a rarity. Previously named as Phialophora parasitica , it was first reported in 1974 to cause subcutaneous tissue infection in renal transplant recipient. [1] Since then, only a few cases have been reported in world literature but perhaps underreporting occurs due to incomplete or incorrect identification. [2] Also, some of the cases of subcutaneous infection in otherwise healthy patients are nondramatic in nature and definitive identification of the etiological agent is not pursued. [2] The spectrum of disease caused by P. parasiticum is variable and ranges from subcutaneous infections to fungemia and disseminated disease. [1],[3] Of the many cases reported to date, a majority involve immunocompromised patients. [4] Good outcomes have been achieved with surgical debridement and use of antifungals like amphotericin B, azoles, and flucytosine (FC). Herein, we report a case of subcutaneous tissue swelling in a young 26-year-old female, whose etiology was traced to P. parasiticum. The therapy was successful with surgical debridement, amphotericin B, and itraconazole. Case Report A 26-year-old woman presented with a tender swelling in the left forearm on 6 th September, 2007. Initially, a year back, the patient had noted a small swelling. The swelling gradually increased in size to approximately 8-10 cm X 4-5 cm [Figure - 1]. There was no history of fever or trauma to the affected part. As the swelling increased there was a feeling of heaviness and cosmetic deformity due to which the patient visited our hospital. The patient was nondiabetic, without any other predisposing factors. There were no obvious lesions in other parts of the body. Tissue biopsy was performed which on Hematoxylin and Eosin staining showed fungal hyphae in fibrocollagenous tissue with minimal inflammatory infiltrate consisting of lymphocyte and eosinophils [Figure - 2]. A piece of the biopsy material was cultured on Sabouraud′s Dextrose Agar (SDA) and incubated at 37 oC. Her hematological, renal, and liver function tests were within normal limits. The patient was nonreactive for HIV antibodies. In the meantime, surgical debridement was performed and the patient was started on intravenous amphotericin B. The debridement tissue showed branched septate hyphae on Gomori′s Methenamine Silver (GMS) staining. Colonies appeared on the SDA which were initially yellowish on the obverse, very slow growing, but within three weeks became gray-black in color [Figure - 3] with blackish pigmentation noted on the reverse, which was limited to the colony and no diffusible pigment in the agar. Slide culture from the colony done on Potato Dextrose Agar (PDA) observed after one week of incubation at room temperature [Figure - 4]. showed slender phialides, slightly tapering toward the tip with small conidia, which were thin walled, cylindrical to sausage shaped, 3-6 X 1.2 mm, and grouped together forming a ball. There was no constriction at the base of the phialides. Hence, the fungus was identified as P. parasiticum . The patient responded well to the combined surgical debridement and amphotericin B treatment regime and was later discharged on oral itraconazle prescribed for two months. The patient had no relapse of symptoms at the last follow up. Discussion P. parasiticum is an unusual cause of human disease. It was first reported in 1974 as Phialophora parasitica causing subcutaneous tissue infection. [1] Since the initial description, few cases have been reported in literature. Phaeoacremonium species are chiefly found in the environment of woody plants as enophytes or as agents of plant diseases. [2] In 1996, Crous et al . [5] proposed a new hyphomycete genus Phaeoacremonium with P. parasiticum as its type species. Morphologically, the genus Phaeoacremonium is intermediate between the genera Acremonium and Phialophora . It is distinguished from Acremonium by its phaeoid vegetative hyphae and from Phialophora by its narrow conidigenous cells and the inconspicuous collarets. Morphological distinction from a number of other relatively similar Phaeoacremonium species has been summarized by Mostrel et al . [6] The single most distinct feature of P. parasiticum is the absence of constriction at the base of the phialides, which is present in P. inflatipes. Phialides of P. parasiticum are more spine-like and not constricted at their bases. Other species of Phaeoacremonium have broad phialides. [6] The spectrum of disease caused by P. parasiticum includes subcutaneous infections, [1],[4] eumycetoma, [7] osteomyelitis, [8] arthritis, and disseminated diseases including fungemia and endocarditis. [4] Baddley et al . [4] reported two cases of P. parasiticum . In the first case reported, a 31-year-old woman with aplastic anemia and prolonged neutropenia, presented with persistent febrile neutropenia despite broad spectrum antibacterial therapy with vancomycin and piperacillin plus tazobactam combination. An amphotericin B preparation (5 mg/kg daily) was added to her regimen upon admission. Multiple blood cultures were obtained upon admission and grew mould. The patient remained febrile and on the 12 th day after admission, developed multiple papulonodular skin lesions on the trunks, arms, and legs. Biopsy of the skin lesions showed hyphae on GMS staining. The patient continued to grow mould from blood cultures and died of sepsis two months after admission. Isolates from the blood and skin biopsy grew P. parasiticum. The second case, a 40-year-old man with a history of cardiac transplantation, was admitted with a swollen tender left forearm displaying nodular lesions. Biopsy from tissue and debridement revealed septate hyphae and cultures grew P. parasiticum . The patient received amphotericin B (0.7 mg/kg daily) for two weeks, followed by 200 mg itraconazole daily. The skin lesions healed. The patient died three weeks after admission, due to causes related to the heart disease. In our case, the patient had no predisposing factors as history of organ transplantation or neutropenia, which are commonly reported to be associated with P. parasiticum infection. The ideal treatment for P. parasiticum is not defined and the paucity of cases does not allow for meaningful comparisons of antifungal agents. Agents commonly used in reported cases include amphotericin B, azoles, terbinafine, and 5 FC. On the basis of limited susceptibility data, amphotericin B and azoles may be effective. [4] Surgical debridement appears to be an important aspect of treatment of localized P. parasiticum infection. Among eight reported cases of localized infection in the world literature, [4] seven had surgical intervention. Appropriate treatment is undefined but surgical debridement and use of amphotericin B and extended spectrum triazoles are reported to be associated with relatively good outcomes. In our case, the patient responded well to amphotericin B and surgical debridement. P. parasiticum is found in the environment of woody plants and endophytes or as agents of plant disease. The species have also been isolated from soil. Minute trauma may cause implantation of the pathogen in the body. [6] Surprisingly, our patient did not give history of trauma, probably she might not have noticed minor trauma of the skin. In summary, P. parasiticum is an uncommon cause of fungal infection and its appropriate identification may be difficult. High index of suspicion is required to diagnose the case, so that early treatment can be given to prevent complications, especially among immunocompromised individuals. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09017f3.jpg] [mb09017f2.jpg] [mb09017f1.jpg] [mb09017f4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}