 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
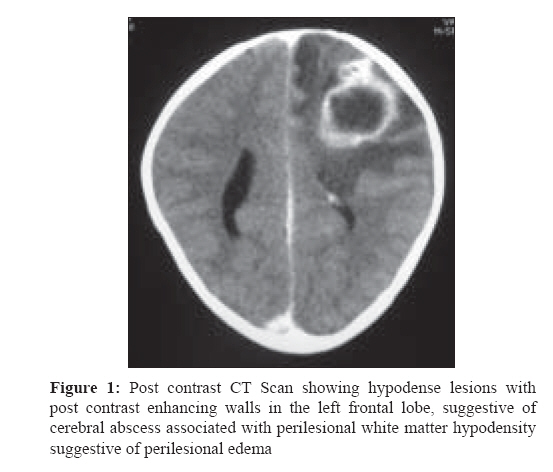
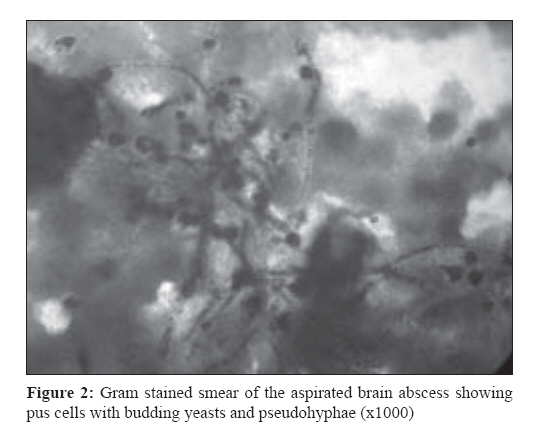
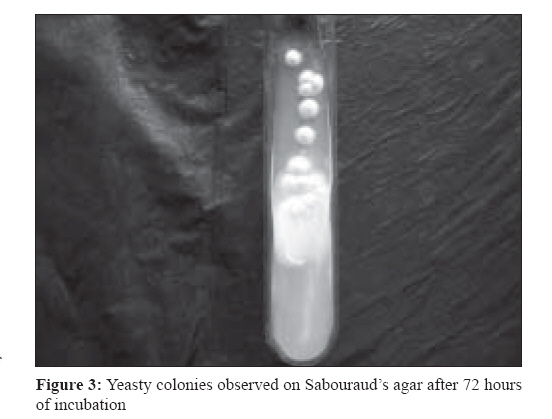
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 70-72 Case Report Cerebral candida abscess in an infant Baradkar VP, Mathur M, Kumar S Department of Microbiology, Lokmanya Tilak Municipal Medical College & General Hospital, Sion, Mumbai-400 022 Date of Submission: 08-May-2008 Code Number: mb09019 Abstract Brain abscess is uncommon in the pediatric population. Here, we report one such case due to Candida albicans in one-year-old infant, without any predisposing factors. The child presented with progressively increasing size of head circumference. The diagnosis was confirmed by CT scan of brain and microbiological investigations on the drained pus material. The patient responded to combination of surgery (drainage) and intravenous amphotericin B. Neurological development six months after hospital discharge was normal. The organism being a rare cause of cerebral abscess in pediatric population is reported here.Keywords: candida , brain abscess Brain abscess is a focal, intracerebral infection that begins as a localized area of cerebritis and develops into a collection of pus surrounded by well-vascularised capsule. [1] They are relatively uncommon. It results from the invasion of infectious organisms into the brain parenchyma as a consequence of the spread of contiguous infection from nonneural tissue, the result of hematogenous introduction from a remote site or direct mechanical introduction due to penetrating trauma or a surgical procedure. [1],[2],[3],[4],[5],[6] Predisposing factors identified include congenital heart diseases; infection of middle ear, mastoids, paranasal sinuses, and soft tissue of the face, orbit, or scalp; insertion of ventriculoperitoneal shunt (V-P) shunts; congenital lesions of head and neck, including dermal sinuses, usually located over posterior fossa; abnormalities of the immune system; low birth weight; leukemia; and organ transplantation. [1],[2],[3],[4],[5],[6],[7] In some cases, no predisposing factors or source of infection can be found. [7] A number of studies have characterized the natural history of intracranial abscess in children. These previous studies documented that intracranial abscess often cause significant morbidity, including epilepsy, motor or sensory dysfunction, visual field defects, and personality changes. [7],[8] Insidious onset and life-threatening complications from increased intracranial pressure and irreversibility of cerebral tissue damage may account for poor prognosis in some cases. [5] Here, we report a rare case of cerebral abscess due to Candida albicans in an infant. Case Report A one-year-old female child presented with a history of fever, increased head circumference, lethargy and poor feeding for one month. There was no history of convulsions, vomiting, trauma, rash, sinusitis, otorrhaea, and no infective focus at other sites. BCG scar was present. The child was preterm, delivered vaginally at 30 weeks with a birth weight of 2000 g. She was not HIV seropositive and the blood sugar was within normal limits. On examination, the child was conscious, lethargic, and had pallor. There was no oral thrush or difficulty on deglutition. The head circumference was 47 cm. The heart and respiratory rates were 120/min and 30/min, respectively, and the blood pressure was 100/80 mm Hg. Abdominal and cardiorespiratory examination were unremarkable. There was no papilloedema on fundoscopy. Routine laboratory investigations showed Hb-9.3 gm/dL; total leukocyte count, 10,300 with 67% polymorphs, 33% lymphocytes, and 5.2 lacs platelets. Serum Na + , K + , Ca 2+ , total bilirubin, direct bilirubin, AST, alkaline phosphatase, total protein, and BUN were all within normal limits . The mother and baby were not seropositive for HIV antibodies. CT scan revealed an intracerebral abscess with midline shift, without signs of meningitis [Figure - 1]. The CSF examination was normal and showed no growth on culture. The abscess was drained under anesthesia, and revealed frank pus. Gram stain of the pus showed plenty of pus cells and budding yeast cells with pseudohyphae (x 1000) [Figure - 2]. The Z-N stained smears did not reveal any acid fast bacilli. The sample was cultured on blood agar, chocolate agar, MacConkey′s medium, Sabouraud′s dextrose agar (SDA), thioglycollate medium and Lowenstein-Jensen medium with and without antibiotics. After 24 hours of incubation at 37 oC, tiny yeasty colonies were observed on the SDA [Figure - 3] and blood agar. The fungus was confirmed to be Candida albicans by the germ tube test, growth on cornmeal agar, tobacco agar and sugar assimilation tests. There was no growth either on the MacConkey agar or on Lowenstein Jensen′s media even after a prolonged six-week incubation period. There were no anaerobic organisms isolated from the thioglycollate medium. The blood and urine cultures did not reveal growth on SDA, blood agar, and MacConkey agar. The oral, throat swabs and stool showed no fungal growth. Antifungal therapy was initiated with intravenous amphotericin B based on the primary smear report. Following drainage of the abscess and antifungal therapy, the patient responded after one month. A repeat CT scan then showed complete resolution of the abscess. After discharge from the hospital the patient was continued on oral fluconazole for six weeks. Neurological development six months after hospital discharge was normal. Discussion Etiology of brain abscess can be bacterial or fungal. Bacteria reported to cause brain abscess in paediatric age group are Streptococcus spp. , Peptostreptococcus spp. , Staphylococcus aureus , Haemophilus infuenzae, E. coli, Klebsiella spp. , Enterobacter spp. , Citrobacter spp. , Proteus spp. , Morganella spp. , Pseudomonas spp. , Bacteroides fragilis, Nocardia spp., and Listeria monocytogenes. [1],[2],[3],[4],[5],[6],[7],[8] Yeasts such as Candida spp. , Cryptococcus neoformans , and other fungi-like Aspergillus spp. have been implicated in 1-17% cases of brain abscess. [1],[5] Neurological signs and symptoms reported in cases of brain abscess include headache, vomiting, photophobia, fever, seizures, and mental status changes. Other neurological findings include parasthesis , dysphagia, dysarthria, aphasia, weakness, hemiparesis, nystagmus, developmental regression, signs of focal neurological deficit or signs of meningeal irritation, and increase in the circumference of the head. [1],[2],[3],[4],[5],[6],[7],[8] In this case, only fever, lethargy, and increased head circumference were the presenting features. Diagnosis of clinically suspected cases of brain abscess is aided by imaging studies such as CT or MRI scanning. Aspiration provides the clinical specimen for the diagnosis by culture, which provides the best opportunity to make a microbiological diagnosis. We would like to emphasize the importance of obtaining pus from brain abscesses, whenever possible, for definitive diagnosis and the optimal therapy, especially when there is no obvious predisposing factor. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09019f3.jpg] [mb09019f1.jpg] [mb09019f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}