 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
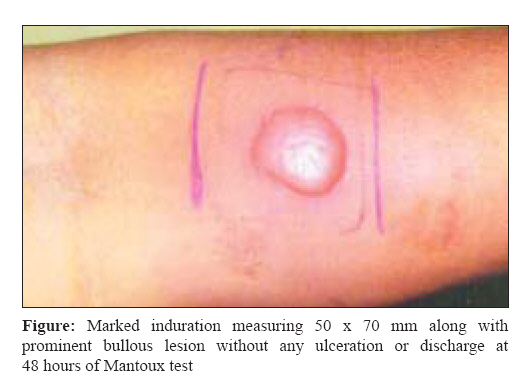
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 78-79 Correspondence Giant mantoux reaction Avasthi R, Chaudhary SC, Mohanty D Department of Medicine, University College of Medical Sciences and Guru Teg Bahadur Hospital, Delhi Date of Submission: 18-Jun-2008 Code Number: mb09022 Dear Editor, Role of Mantoux test in diagnosis, though limited, cannot be underestimated in immunocompetent patients with an average nutritional status. Most persons likely to have positive reaction develop mild erythema, induration, and itching by 24 hours. The positive reaction peaks at 48-72 hours with an area of erythematous induration that resolves within a week. We describe below a patient who developed a very large lesion after Mantoux testing. A 45-year-old woman presented with intermittent, low-grade fever associated with headache since three months. There was no history of vomiting, cough, hemoptysis, weight loss, seizure, altered sensorium, or any anesthetic skin lesion. The patient denied any family history of either tuberculosis or leprosy. General physical and systemic examinations were normal, except a single tender lymph node approximately 1 x 1 cm in the left axilla. Examination did not reveal any thickened nerve. The hemogram, liver and kidney function tests, blood sugar and urine examination were normal. Venereal Disease Research Laboratory (VDRL) and enzyme linked immunosorbent assay (ELISA) for human immunodeficiency virus (HIV) were nonreactive. Chest radiograph did not show infiltration/adenopathy and abdominal ultrasound was normal. Erythrocyte sedimentation rate was 76 mm in the 1 st hour. Fundoscopy did not show any papilloedema. A Mantoux test was done by intradermal injection of 0.1 ml purified protein derivative (PPD) containing 5 tuberculin unit (0.1 µg standard PPD) on the anterior aspect of forearm. Patient started developing marked erythema and induration within 6 hours. By 48 hours she developed a red lesion with marked induration measuring 50 x 70 mm along with a prominent bullous lesion without ulceration or discharge [Figure - 1] This massive lesion persisted for nearly two weeks. A fine needle aspiration cytology of the left axillary lymph node showed evidence of granuloma and necrosis along with acid fast bacilli (AFB). She was diagnosed as tubercular lymphadenitis and started on category III antitubercular regimen comprising of rifampicin 450 mg, isoniazid 300 mg, ethambutol 800 mg, and pyrazinamide 1000 mg daily for initial two months during intensive phase followed by rifampicin 450 mg and isoniazid 300 mg daily for four months during continuation phase. Patient showed remarkable improvement of symptoms within a month of treatment with regression of lymph node size and is completely asymptomatic at present on completion of antitubercular therapy. This patient demonstrated a very massive response following Mantoux testing including an immediate erythematous reaction by 6 hours, the largest seen by us. This is an uncommon phenomenon since tubercular response is a delayed type of hypersensitivity reaction. This early reaction is common in patients with active pulmonary tuberculosis and heavy mycobacterial antigen load, or sometimes as a result of frequent contacts with tuberculosis patients and rarely as a hypersensitivity phenomenon. [1] It is also well known that strong reactors particularly those with induration> 20 mm have more chances of developing active tuberculosis than those with the commonly defined 10 mm induration. [2] An exaggerated response causing giant reaction to tuberculin has been occasionally described in patients with lepromatous leprosy. Although the mechanism is not clearly understood, it is suggested that a coincidence of delayed hypersensitivity to tuberculin and a less delayed phenomenon of excessive local edema due to systemic features may be responsible for these changes. A temporary lack of immune regulation along with changing level of antigenic load has been advocated as the cause for such giant reaction in lepromatous leprosy. [3] Despite limitation of tuberculin testing in developing countries, it is a useful test for assessing the prevalence of tuberculosis infection in the community. The adage that the tuberculin test should be approached with respect, administered with care, read with deliberation, and interpreted with caution seems extremely appropriate. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09022f1.jpg] |
| |||||||||
{kind=link}