 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
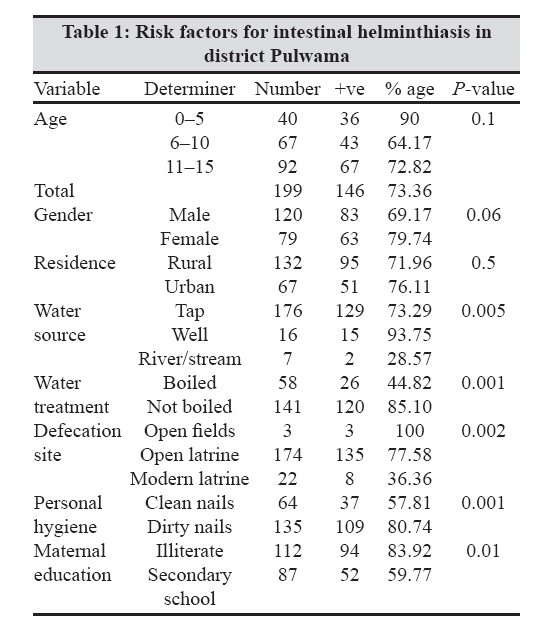
Indian Journal of Medical Microbiology, Vol. 27, No. 1, January-March, 2009, pp. 81-82 Correspondence Intestinal helminths and associated risk factors in children of district Pulwama, Kashmir, India Wani SA, Ahmad F PG Department of Zoology, University of Kashmir, Srinagar-190 006 Date of Submission: 06-Apr-2008 Code Number: mb09025 Dear Editor, Helminth infestation is highly prevalent throughout the developing countries of the world. The aim of the present study was to determine the prevalence of intestinal helminth infestation in school children of Pulwama district, Kashmir, India, and to assess the associated epidemiological factors. Stool samples were collected from 199 students enrolled in eight middle level schools, which were processed by using both simple smear and zinc sulphate concentration method and microscopically examined for intestinal parasites. Of the 199 students surveyed, 73.36% had one or more intestinal helminths. Prevalence of Ascaris lumbricoides was highest (69.84%), followed by Trichuris trichiura (31.65%), Enterobius vermicularis (16.80) and Taenia saginata (3.01%). Conditions most frequently associated with infestation included the water source, defecation site, personal hygiene and the extent of maternal education. Among the intestinal parasitic infections, helminth infestations are the most common in the Indian subcontinent. There are few hospital-based studies on the prevalence of intestinal parasites in Kashmir, [1] which may not be a true indicator of their prevalence as asymptomatic children may have been missed. The present study was undertaken to determine the prevalence of gastrointestinal helminths among school children of Kashmir valley, India. Pulwama is located about 2000 m above sea level. The population density in the city is 356/km. [2] The study was carried out in both, urban as well as rural areas, from April to October 2007 in eight middle level schools located in Pampore, Ratnipora, Kakapora, Tral, Shopian, Galandar, Trehama and Awantipora localities of Pulwama district. In all, 199 asymptomatic children aged between 5 and 14 years (mean = 9.1±2.8 years) and not on antiparasitic treatment were included. Written consent was obtained from both parents. Children requiring medical assistance were either treated or referred for medical attention. The study population was further divided into three age groups, i.e. 1-5, 6-10 and 11-15 years. The socioeconomic data of the children′s families was collected with a structured questionnaire. The interviews were held face to face with the mothers, at the schools. The level of education of the mother, sanitary facilities, source of drinking water (tap, well or river/stream) and defecation site (open or modern sanitary latrine) were queried for as indicators of the socioeconomic condition. The age of the children was obtained from school records. After collecting a stool specimen, the containers were labeled and immediately transported to the Parasitology Laboratory, Department of Zoology, University of Kashmir, and were processed using direct smear and zinc sulphate concentration technique. All the helminths found were identified. Statistical analysis was carried out by Chi square test. Stool examination of 199 children revealed the presence of at least one intestinal helminth in 146 (73.36%) children.Of the study population, 69.84% was infested with Ascaris lumbricoides followed by Trichuris trichiura (31.65%), Enterobius vermicularis (16.80%) and Taenia saginata (3.01%). Of the study population, 32.16% were infested with a single and 41.20% with multiple infestations. Prevalence of infestation was highest in the age group of 0-5 years (90%), followed by 11-15 years (72.82%) and 6-10 years (64.17%). Risk factors related to intestinal helminthiasis are summarized in [Table - 1]. The present study indicated a relatively high prevalence of intestinal helminths in the school children of Pulwama district. Studies conducted on the frequency distribution of gastrointestinal helminths in Malaysia showed a high overall prevalence of 62% among the urban slum children. [2] In Maracaibo, Venezuela, a high prevalence of 72% was reported among the school children studying in a public institution. [3] The high prevalence in Pulwama district is probably a consequence of a low standard of living, poor sanitation, lack of personal hygiene, traditional methods of agriculture, indiscriminate defecation, use of night soil as fertilizers and other occupational hazard. Even though gender was not a significant risk factor for prevalence of intestinal parasitic infections, females were more likely to be infected (79.74%) than males (69.17%). This can be partially explained by the difference in gender behaviour. Girls are likely to perform unhygienic tasks like carrying night soil and cow dung in baskets to the fields. Male children seldom perform these tasks due to social restrictions. Also, in these areas, girls are seldom admitted to schools because of religious implications and hence they know little about maintaining personal hygiene. Children drinking water from wells were found to have a greater prevalence of infection than those who had access to tap water. This pattern of infection has been confirmed in different studies. [4] Poor hygiene practices associated with access to water is a highly probable risk factor for increased parasitic infestation among children. It is also evident that children with better personal hygiene had a lower prevalence of intestinal helminth infestations than those living in less hygienic conditions ( P < 0.01). In our study, maternal education was a significant risk factor i.e. prevalence of infection decreased as the level of maternal education increased. Apparently, this factor extensively contributes to controlling risk factors for intestinal infections. Maternal education has been found to be the most important risk factor for parasitism in other studies as well. [5] The present study reveals that intestinal helminths are abundant among school children of Pulwama district. This situation strongly calls for control measures, including treatment of infected individuals, improvement of sanitation practices and provision of clean water. The impact of each measure would be maximized through a health education program directed at school children and their mothers in particular, and to communities in general. Acknowledgements Financial support: Department of Science and Technology (J & K Government)References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09025t1.jpg] |
| |||||||||
{kind=link}