 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
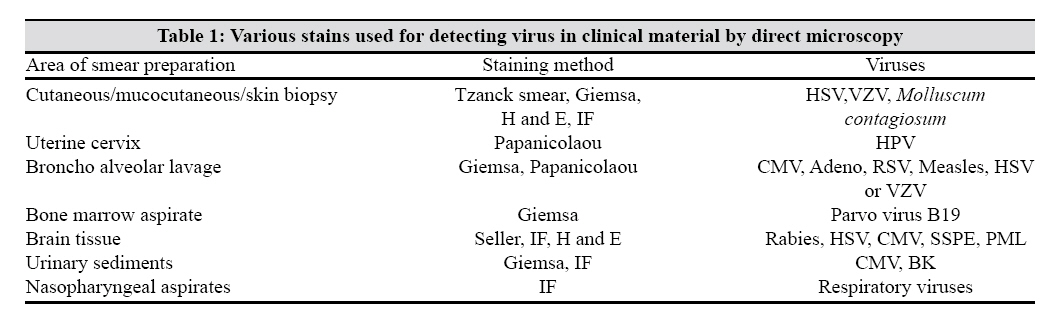
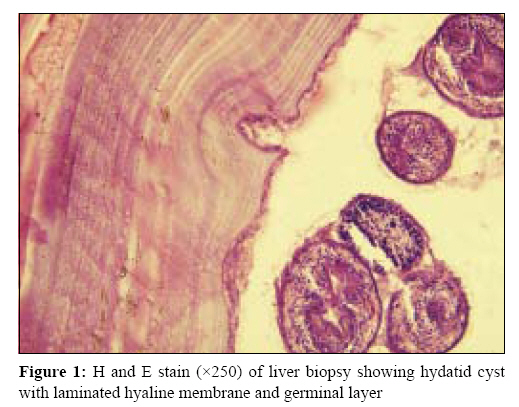
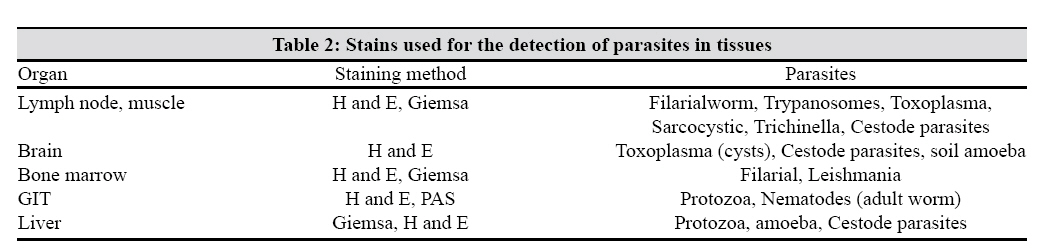
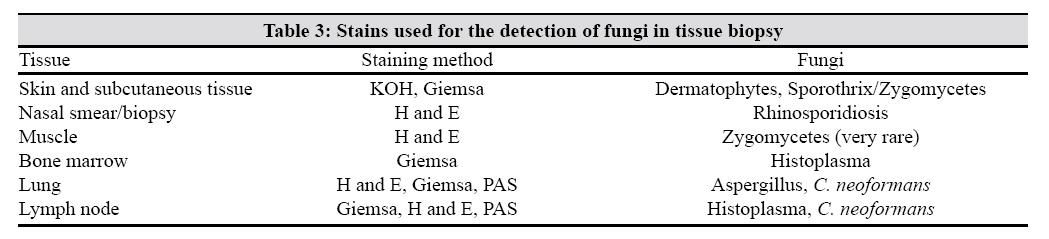
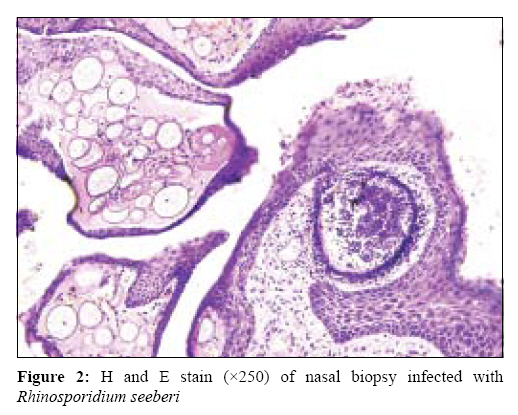
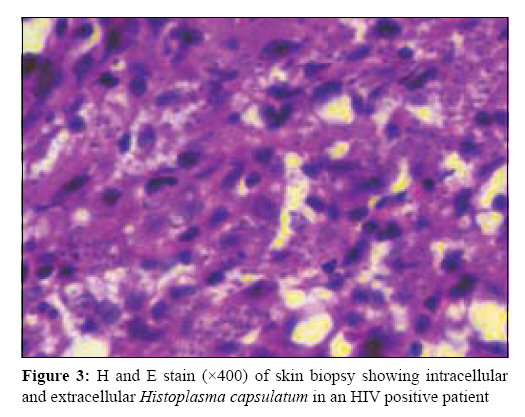
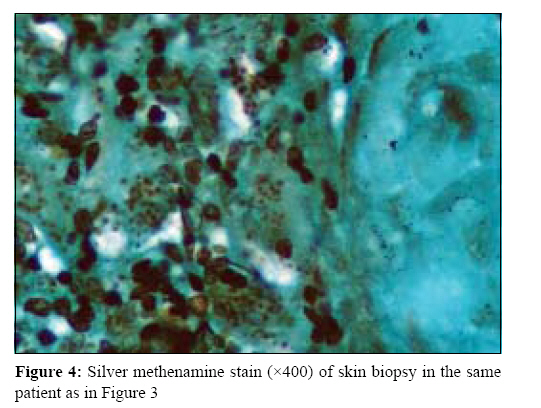
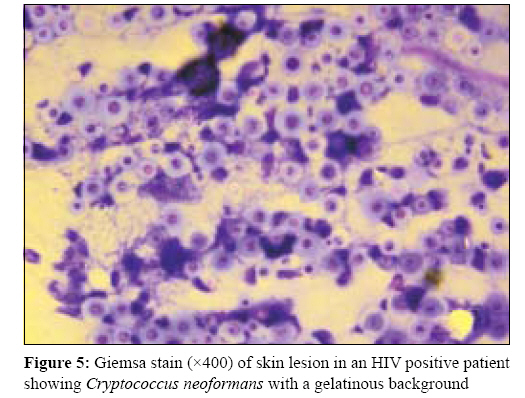
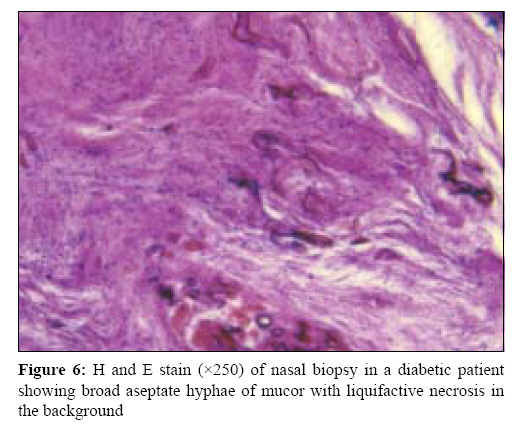
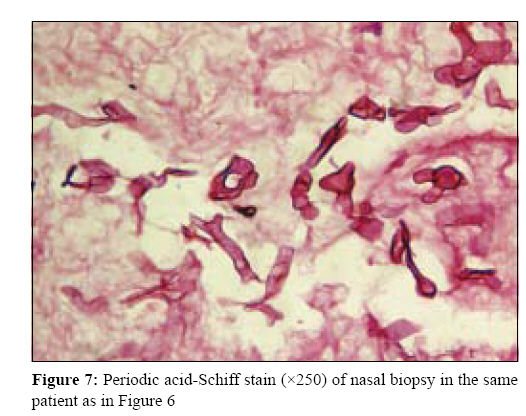
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 100-106 Review Article Histopathology for the diagnosis of infectious diseases Gupta E, Bhalla P, Khurana N, Singh T Department of Microbiology, Maulana Azad Medical College (MAMC), New Delhi - 110 002 Date of Submission: 06-Aug-2008 Code Number:mb09034 PMID: 19384030 DOI: 10.4103/0255-0857.49423 Abstract Histopathological examination of tissue biopsies for the identification of infectious organisms is a very important diagnostic tool. Conventional culture confirmation of tissue biopsies often fail to identify any pathogen as, first of all, invariably most of the tissue samples that are collected and sent for culture isolation are inappropriately collected in formalin, which prevents pathogen growth in culture media. Inadequate processing like grinding, etc. further hinders isolation. Presence of inhibitors like dead tissue debris, fibers, etc. also delays isolation. Microbiologists often lack expertise in identifying infectious pathogens directly from tissue biopsies by microscopic visualization. This review therefore acquaints microbiologists with the various methods available for detecting infectious agents by using histological stains. On histopathological examination of the tissue biopsy once, it is determined that a disease is likely to be due to an infection and has characterized the inflammatory response and hence associated microorganisms should be thoroughly looked for. Although some microorganisms or their cytopathic effects may be clearly visible on routine haematoxylin- and eosin-stained sections, additional histochemical stains are often needed for their complete characterization. Highly specific molecular techniques, such as immunohistochemistry, in situ hybridization and nucleic acid amplification, may be needed in certain instances to establish the diagnosis of infection. Through appropriate morphologic diagnoses and interlaboratory communication and collaboration, direct microscopic visualization of tissue samples can thus be very helpful in reaching a correct and rapid diagnosis.Keywords: Histopathology, infections, tissue biopsy Conventional isolation of the aetiological agent by culture followed by its identification is the best way to identify any pathogen to establish infectious disease aetiology in any disease. Because of a number of reasons, e.g., improper specimen collection, transportation and processing, there is a poor isolation rate of microorganisms from cultures in tissue biopsies. The histopathology of infectious diseases, i.e., direct microscopic visualization of tissue samples for identification of the infectious agent, is particularly useful when cultures cannot be made or the infectious agent is slow growing or fastidious. [1],[2] Direct microscopy before culture is an added tool to culture findings; however, it cannot totally replace conventional methods. Many infective agents cause typical tissue responses that may vary as the infection progresses from acute to chronic or disseminated phases. When considered with relevant clinical information, the histological features seen in tissue biopsies may provide sufficient information to correctly identify a particular type of organism. [3],[4],[5] Pathologists are well versed with histopathology for infectious diseases. Microbiologists often lack knowledge regarding the direct microscopic visualization of infectious agents in tissue biopsies. The goal of this review is to acquaint microbiologists with the methods available for detecting infectious agents by using histological stains. It is indeed essential for a microbiologist to be able to identify a pathogen by looking at the characteristic histopathologic features and applying the correct identification techniques for the pathogen of interest. In recent decades, advances in molecular biology have led to methodologies that will specifically identify many organisms correctly at the tissue level. Understanding the histopathologic methods enables the clinical microbiologist and pathologist to communicate effectively, hopefully leading to an earlier, more precise diagnosis of patient disease. Advantages of the Microscopic Visualization of Tissue Sections Before Culture Culture alone cannot distinguish between colonization and true tissue invasion. Microscopy often adds a lot of information, e.g., if Candida albicans is isolated from a sputum culture, it does not necessarily indicate that the organism is causing pneumonia unless pseudohyphae, budding yeasts or both invading the lung parenchyma are also seen on the direct microscopy. Isolation of Pseudomonas aeruginosa from a burn wound specimen may represent a life-threatening situation or colonization of the wound. Microscopic examination of tissue from the burn wound site reveals whether gram-negative bacilli are present only in the dead tissue or have invaded the viable tissue. If invasion is seen, true pathogenecity is actually represented. [6] In certain situations, changes in the host tissue histology with or without the actual presence of pathogen would hint at the type of infection. For example, presence of caseous granulomas hints to the infection by Mycobacterium tuberculosis . [7] Similarly, tissue infiltration with a particular type of cell, e.g., eosinophil, would go for parasitic infection. [8] Sometimes even the histopathological changes within a tissue will lead to a probable diagnosis, like in the case of Human papilloma virus (HPV) infection, where a probable diagnosis is made by a PAP smear examination of the cervix. [9] Other situations in which evaluation of smears and tissue sections stained for organisms are useful include those when multiple organisms are cultured. When several organisms are cultivated, the morphology of the predominant organism visualized in the tissue sections can suggest the true causative agent. It is also useful especially in the diagnosis of infection caused by non-cultivable agents such as M. leprae , Pneumocystis carinii , Treponema pallidum , the Whipple′s disease bacterium ( Tropheryma whipplei ) and Loboa loboi . Microscopic evaluation yields a more timely diagnosis for diseases caused by organisms that are difficult to culture (e.g., rickettsiae) or fastidious organisms like Coxiella and Bartonella. [10] In situations when specific morphology of the pathogen is characteristic, microscopy acts as a very rapid diagnostic assay, e.g., demonstration of Leishmania donovani (LD bodies) in splenic or bone marrow aspirates.Host Inflammatory Response Inflammation is the hallmark of most infectious diseases. It may also be associated with neoplasia, dysplasia, autoimmune diseases, allergic conditions and idiopathic disorders such as Wegener′s granulomatosis and sarcoidosis. Many of these non-infectious disorders are treated with corticosteroids, the inappropriate use of which may exacerbate infection. Therefore, it is critical for both the histopathologist and the microbiologist to be able to differentiate between inflammatory conditions caused by infectious agents from those with non-infectious aetiologies. [11] Once it is determined that an inflammatory response is likely due to infection, the next step is to find out which aetiologic agents are the possible causes of the infection. Although the inflammatory response may vary in different individuals, broadly one type of pathogen usually elicits one particular type of response, e.g., in bacterial infection, infiltration of the tissue with polymorphs predominates whereas in viral infections, it is replaced by lymphocytic infiltration. [3],[11]Various Histochemical Stains for Infectious Disease Pathology The haematoxylin-eosin (H and E) stain is the most common stain for the histopathologic evaluation of tissue sections. Although many microorganisms can be visualized in H and E-stained sections, others can be visualized only with special histochemical stains. [3],[4] The most common special stains for microorganisms are the tissue Gram stain for bacteria (of which there are several common variants), [12],[13],[14],[15] the Grocott-Gomori methenamine silver stain (GMS) for fungi and the Ziehl-Neelsen (ZN) and Kinyoun acid-fast stains for mycobacteria and nocardia. Other histochemical stains for detecting or identifying microorganisms include the periodic acid-Schiff (PAS) stain for fungi, mucicarmine and alcian blue stains to demonstrate the capsule of Cryptococcus neoformans , the Giemsa stain for parasites and fungi and silver stains such as the Warthin-Starry, Steiner and Dieterle stains for bacteria. [3],[4] These histochemical stains are useful for detecting the majority of human pathogens, but limitations in specificity exist and special conditions warrant additional diagnostic techniques. Sensitivity of special stains to detect pathogens depends on a number of factors like number of microorganisms present at the site, technical factors associated in sample procuring, observer′s capability, magnification used and finally availability of specific confirmatory tests. Highly specific molecular techniques, such as immunohistochemistry, in situ hybridization and nucleic acid amplification, may be needed in certain instances to further confirm the diagnosis. Thus, through appropriate morphologic diagnoses, a microbiologist can contribute greatly to the timely diagnosis of infectious diseases.Diagnosis of Viral Infections Viruses induce characteristic morphologic changes during their replication in the cells they infect. Morphologic features indicative of a viral infection include the formation of inclusion bodies in the host cell nucleus, cytoplasm or both. For some viruses, formation of multinucleate giant cells, presence of a perinuclear halo around the infected cell, lymphocytic infiltration or even cellular necrosis can be useful. The three most commonly recognized viral infections by histopathological changes are those caused by herpes simplex virus (HSV), cytomegalovirus (CMV) and HPV. [9],[16],[17] The Tzanck smear (smear prepared from the base of the vesicle) is useful for the rapid diagnosis of cutaneous or mucocutaneous lesions caused by HSV or varicella zoster virus infection. Other stains useful in viral infection include Giemsa stain, especially for CMV infection to look for the presence of inclusion bodies (owl′s eye appearance) and Sellar stain for Rabies virus infection [Table - 1]. Demonstration of giant proerythroblasts in Giemsa- stained smears of the bone marrow are often diagnostic for Parvovirus B19 infection. [18]Diagnosis of Parasitic Infections The specimen most frequently submitted for detection of parasites is stool and the usual request is examination for ova and cyst. Apart from a saline mount and iodine-stained wet mount, modified ZN stain or Kinyoun stain is used in addition for Cryptosporidium, Cyclospora and Isospora, especially in immunocompromised patients. Specimens other than stool submitted for detection of parasites include peripheral blood film (thick and thin smear), bone marrow smear, duodenal aspirates, sputum samples, skin, muscle biopsy, etc. The direct wet mount also is a useful first step in the examination of these specimens and if parasites are detected, the specimen is fixed and stained to confirm the diagnosis. Giemsa staining is recommended for detection of many parasites, [19] including blood pathogens ( Plasmodium species, Babesia species, Trypanosoma species, L. donovani and microfilariae) in thick and thin blood films, L. donovani in bone marrow and splenic aspirates and Leishmania species in aspirates or imprints of cutaneous or mucocutaneous lesions, trypanosomes in lymph node imprints, Toxoplasma gondii in imprints of brain, lung or other tissues and G. lamblia , microsporidia and Entamoeba histolytica in imprints of gastrointestinal biopsy. Tissue stains like H and E [Figure - 1] and PAS help not only in the identification of the parasite (tissue nematodes, Toxoplasma) but also in the visualization of cellular morphology [3],[4] [Table - 2].Diagnosis of Fungal Infections Histopathology remains one of the major tools of diagnosis in mycology [20] [Table - 3]. The major advantages of histopathology are speed, low cost and the ability to provide a presumptive identification of the infecting fungus as well as demonstrating the tissue reaction. However, unless special techniques such as immunofluorescence are used, or the infecting fungus possesses unique structures such as spherules, definitive species identification of the aetiologic agent by histopathology is difficult. Nevertheless, it usually provides essential information before the fungus can be isolated in a mycology laboratory. Furthermore, histopathology is the only way to diagnose infections caused by L. loboi or Rhinosporidium seeberi [Figure - 2] as cultivation techniques have to date been unsuccessful. A number of histologic stains are available that are routinely used to visualize fungi in tissue sections. [21],[22] While some of these are special fungal stains, others are of more general use and still help to observe the tissue reactions and/or the infecting fungus. GMS, Gridley′s fungus and PAS are very efficient to visualize the fungi. Among these three, GMS is more advantageous because it stains old and non-viable fungal elements more efficiently than the other two. H and E stain, on the other hand, is very useful to visualize the host′s response but is not a special fungal stain. It does not stain most of the fungi, except the Aspergillus spp. and the Zygomycetes. Thus, a combination of GMS and H and E is usually employed to visualize both the tissue reaction and the infecting fungus [Figure - 3] and [Figure - 4]. Mucin stains, like Mayer′s mucicarmine, and Alcian blue stain the mucopolysaccharide capsule of C. neoformans . Blastomyces dermatitidis and R. seeberi may also be stained with the mucin stains. Achieving a successful histopathologic diagnosis begins with selection of the tissue sample to be examined. While some fungi are more readily located at the periphery of the infected lesion, others are more prominent at the centre. The major growth forms of the fungi that help in histopathologic diagnosis are the yeast cells [Figure - 5], hyphae [Figure - 6] and [Figure - 7], pseudohyphae, arthroconidia, chlamydoconidia and spherules. The characteristics of each of these (shape, size, location and colour) help in identification of the fungus. Tissue components such as Russell bodies, calcified bodies, elastic fibres and small blood vessels may resemble fungi. Careful examination by experienced specialists significantly reduces such an over diagnosis. The KOH preparation is used primarily for visualizing unstained fungal elements in skin, hair and nails and in specimens, such as sputum and vaginal secretions that contain large amounts of cellular material, because KOH dissolves keratin and much of the other interfering background protein-rich debris. Many laboratories have substituted calcofluor white for KOH or use a combination of the two reagents. Calcofluor white is a fluorescent brightener or whitening agent that binds to cellulose and chitin in fungal cell walls and fluoresces with a blue white colour when exposed to ultraviolet radiation. India ink preparation is used for the diagnosis of C. neoformans in cerebro spinal fluid samples.Diagnosis of Bacterial Infections Bacteria are the most difficult microorganisms to detect in routine H and E-stained histologic sections. Tissue diagnosis of a bacterial infection begins with the recognition of a consistent pattern of inflammation. Individual bacteria are generally not detected in H and E-stained tissue sections. Granules can be visualized by H and E stain in cases of actinomycosis. Several modifications of Gram stains can be used for the detection of bacteria in tissue sections. [14],[15] Gram-negative bacteria are particularly difficult to visualize, mainly because of a lack of contrast between the bacteria and the counter stain. The Brown-Brenn tissue Gram stain is preferred for the detection of gram-positive bacteria whereas the Brown-Hopps modification is superior for the detection of gram-negative bacteria. Some bacteria, such as Legionella species, Bartonella species and the spirochetes, stain weakly or not at all with tissue Gram stains. Silver precipitation stains, such as the Warthin-Starry, Steiner or the Dieterle stains, may be used to detect these bacteria. [3],[4] Tissue sections stained by use of silver precipitation techniques should be correlated with the tissue Gram stain because the silver precipitation techniques are non- specific and will stain any bacterium that is present. Any excess silver precipitate makes interpretation difficult or impossible because collagen, fragmented elastin fibres, mucin, neutrophil granules and cytolytic debris stain with silver precipitation techniques. Various other special stains have proven useful for detection of selected bacteria in tissue sections. H. pylori may be demonstrated with modified Giemsa, acridine orange, Wright-Giemsa or toluidine O, but none appear to be as sensitive as the Warthin-Starry stain. [23],[24] Histopathological diagnosis of mycobacteria is quite common and staining procedures most commonly used for visualization of these acid fast bacilli in smears are ZN and Auramine O. Tissue diagnosis of a mycobacterial infection begins by examination of H and E-stained tissue sections. Although organisms cannot be seen, the pattern of granulomatous inflammation provides the first indication that mycobacteria should be considered among the differential diagnoses. [3],[7] Newer Techniques: Immunohistochemistry, In Situ Hybridization and In Situ Polymerase Chain Reaction (PCR) Molecular assays increase the specificity and in some instances may increase the sensitivity of histopathologic tests. [25],[26] Molecular methods of detection may be particularly useful when microorganisms are undetectable by means of histochemical staining methods, are present in low numbers, stain poorly, are uncultivable or exhibit an atypical morphology. [27] In some cases, molecular methods are important for the rapid, specific and quantitative detection of microorganisms. These methods are also useful for differentiating between morphologically similar microorganisms as seen on routine histopathology. Fluorescent in situ hybridization (FISH) is a technique that can be used to detect and localize the presence or absence of specific DNA sequences on chromosomes. It uses fluorescent probes that bind to only those parts of the chromosome with which they show a high degree of sequence similarity. Fluorescence microscopy is used to find out where the fluorescent probe is bound to the chromosome. FISH is often used for finding specific features in DNA. These features can be used in genetic counselling, medicine and species identification. FISH using rRNA-targeted oligonucleotide probes is widely used for the investigation of uncultured bacteria in complex microbial communities and has recently also been shown to be a valuable tool for the rapid detection of various bacterial pathogens. Although it is most commonly used to detect viral targets, FISH has also been used to detect common bacteria and fungi as well as intracellular bacteria such as Chlamydia pneumonia and Rickettsia species. [30] Nucleic acid amplification methods that use tissue sections include in situ PCR and conventional amplification methods using tissue extracts. In situ PCR is a method that may be used to amplify the nucleic acid of a specific target by use of PCR in an intact tissue section to detect and localize the amplified product. This method has been used to detect viruses in tissue sections. [31] It is, however, technically difficult to perform and prone to contamination because amplification occurs on a slide rather than in a closed tube. Contaminants and Artifacts Contamination of tissue sections with organisms, particularly bacteria and fungi, and their subsequent demonstration with routine and special staining methods is a potential cause of false positivity and misdiagnosis. Contamination may occur during several stages of tissue processing, cutting and staining. The most common source of contamination involves the section flotation bath, which is normally set between 45°C and 50°C and provides an environment for bacteria, algae and fungi to grow. Tap water, which may contain a variety of organisms, should not be used in flotation baths. Fresh distilled water should be used and changed at the start of each day. Baths should be cleaned daily and left empty overnight. Bacteria and fungi will also grow in buffers, reagents and stains kept at an ambient temperature for long periods. Contamination of mounted tissue sections from washing or staining solutions will deposit organisms on top of the sections and above the focal plane of the section. Generally, deposition of organisms onto or under tissue sections will be randomly distributed and not confined to areas of pathological significance or even to the section itself. If a contaminant is suspected, stains should be repeated after any potential sources of contamination have been discarded and reagents freshly prepared. Tissue specimens may also be contaminated with bacteria before fixation. If fixation is delayed or avoided, growth may occur on exposed surfaces and this would be reflected in the tissue section. Autopsy specimens are particularly prone to post-mortem bacterial and fungal growth, especially in the respiratory and alimentary systems. Some staining methods, such as Gram′s stain, may produce artefactual deposition of fine dye crystals, which may mimic bacterial rods. Usually, polarised light will reveal these deposits to be refractile and, therefore, artefactual. Conclusion The utility of histopathology in the diagnosis of infectious disease has been well established. Microscopic identification of a pathogen by its morphological features on staining continues to be the mainstay of diagnostic histopathology but recent developments in immunohistochemistry and molecular diagnostics will definitely be more rapid and also specific. However, the routine histopathological identification of microorganisms cannot replace conventional microbiologic culture techniques. The successful characterization of the infectious disease pathology requires the proper characterization of the inflammatory response, knowledge of associated pathogens, use of special histochemical stains and, in some instances, use of highly specific molecular technologies. If microbiologists, pathologists and clinicians communicate effectively, timely and often correct diagnosis of many difficult-to-diagnose diseases can be efficiently made. Tissue biopsies should also be submitted for culture and isolation of pathogens and before culture, all biopsies should be examined for the presence of pathogen or suggestive features leading to infection. Important information is often missed if careful microscopic visualization of the tissue sample is not carried out. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09034t1.jpg] [mb09034f3.jpg] [mb09034f4.jpg] [mb09034t2.jpg] [mb09034t3.jpg] [mb09034f1.jpg] [mb09034f5.jpg] [mb09034f6.jpg] [mb09034f7.jpg] [mb09034f2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}