 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
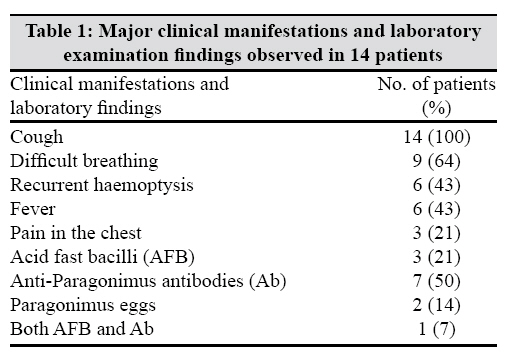
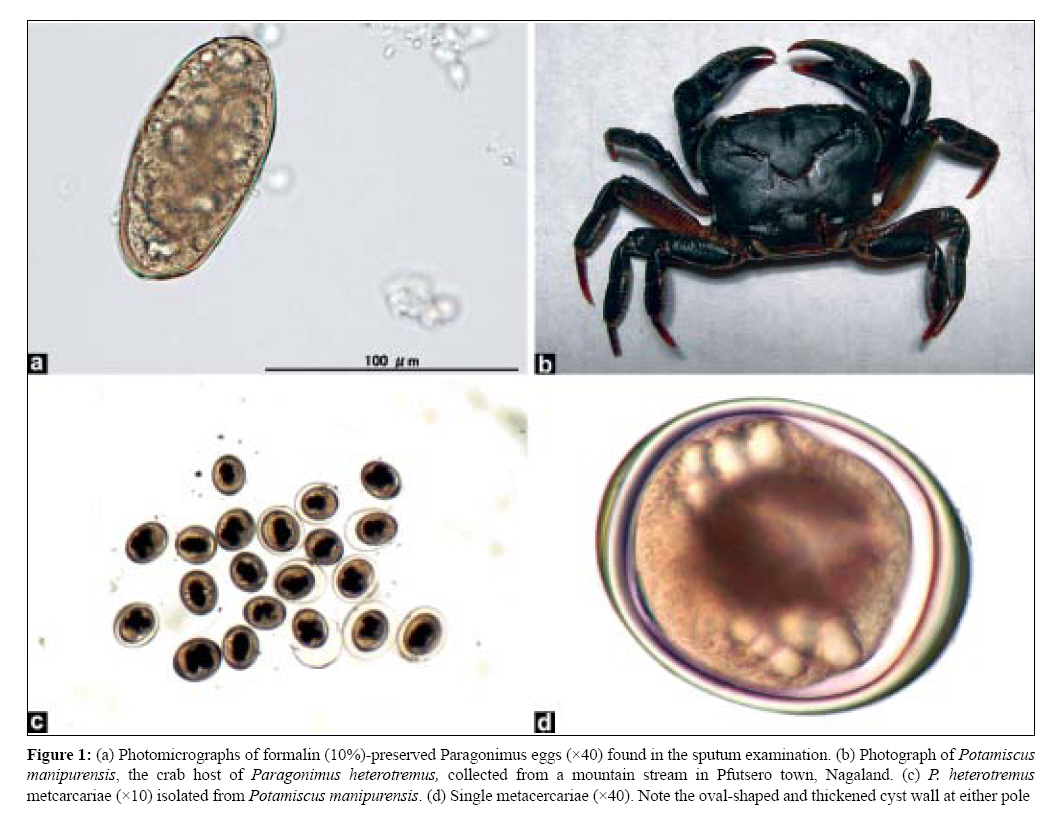
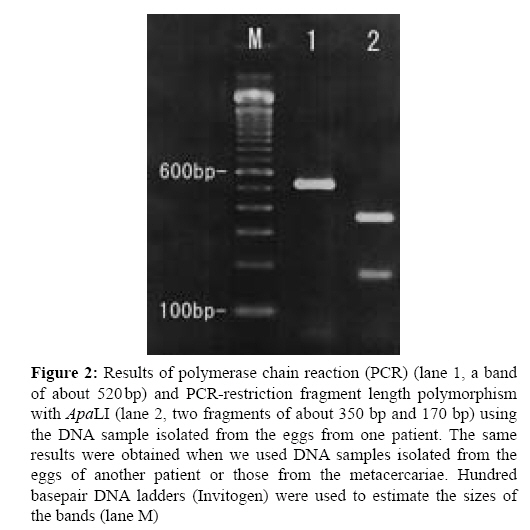
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 123-127 Original Article Paragonimus heterotremus Infection in Nagaland: A New Focus of Paragonimiasis in India Singh TS, Sugiyama H, Umehara A, Hiese S, Khalo K Department of Microbiology, Sikkim Manipal Institute of Medical Sciences, 5th mile, Tadong - 737 102, Gangtok, Sikkim Date of Submission: 19-Aug-2008 Code Number: mb09038 PMID: 19384034 DOI: 10.4103/0255-0857.49424 Abstract Purpose: To determine the prevalence of paragonimiasis among the patients who were attending the tuberculosis (TB) clinics at the Community Health Centre, Pfutsero, Phek District, Nagaland. To determine the species of Paragonimus that cause infection in humans and the crustacean host that acts as the infectious source for humans.Materials and Methods: Sputum specimens were examined microscopically for Paragonimus eggs and acid fast bacilli. Blood samples were tested by microenzyme-linked immunosorbant assay for Paragonimus-specific immunoglobulin G antibodies. Crab extracts prepared by digestion with artificial gastric juice were examined for Paragonimus metacercariae under a stereoscopic microscope. The species identification of the parasite was based on morphological and molecular characterizations of eggs and metacercariae employing polymerase chain reaction and DNA sequencing. Results: Seven out of the 14 patients tested seropositive for paragonimiasis and Paragonimus eggs were detected in sputum of two out of the seven seropositive patients, indicating a prevalence of 50% and an egg detection rate of 14%, respectively. The prevalence was highest in the 10-30 year age group. More males got the infection than females, the ratio being 5:2. P. heterotremus was identified as the causative agent of human paragonimiasis and Potamiscus manipurensis as the crab host. Conclusions: The study revealed that paragonimiasis has been endemic in Pfutsero, Nagaland, and half of the patients attending the TB clinic were actually suffering from pulmonary paragonimiasis. This is the first confirmed report of an endemic focus of paragonimasis and description of P. heterotremus as the causative agent in Nagaland, India. Keywords: India, lung fluke, Nagaland, paragonimiasis, P. heterotremus, tuberculosis Introduction Lung flukes have been described in the world, mainly from East and Southeast Asia and also from Africa and Americas. Paragonimus westermani , the most widely distributed species in Asia, was first described by Kerbert from the lungs of a Bengal tiger, which was captured in India and died at a zoo in Amsterdam more than a century ago. However, very little attention has been paid to this parasite because paragonimiasis was never considered to be a public health problem in India and had remained a neglected disease until the first case was reported from Manipur in 1982. [1] After that, many cases were reported from several parts of Manipur. [2],[3],[4] Subsequently, endemic foci of paragonimiasis were also discovered in Arunachal Pradesh. [5] Most interestingly, P. heterotremus has been identified as the causative agent of human paragonimiasis in this part of India against the widely believed P. westermani , which was reported from many mammals in India. In the past, some occasional cases from Nagaland, initially diagnosed as pulmonary TB by clinical symptoms and chest X-rays, were referred to the Regional Institute of Medical Sciences, Imphal, Manipur. The cases were parasitologically confirmed as pulmonary paragonimiasis. However, detailed information on the prevalence of paragonimiasis in the northeast states of India other than Manipur and Arunachal Pradesh were limited. The present study was, therefore, performed to ascertain the prevalence of paragonimiasis among the patients who were attending the TB clinic at the Community Health Centre, Pfutsero, Nagaland, and to determine the causative species and some of the epidemiological factors responsible for the infection. Materials and Methods Patients and clinical examination The senior author visited the Community Health Centre at Pfutsero town, Phek district, Nagaland, during March 27-28, 2008 to investigate paragonimiasis among the patients attending the TB clinic at the health centre. Pfutsero town is located in southeast Nagaland, bordering Manipur in the south and Myanmar in the east. Detailed clinical history taking and physical examination of all the patients were performed by the medical officers. The findings were recorded in a pre-designed profoma printed in English. Informed consent about the examination and procedures was obtained from each patient after proper explanation in their own dialect. Postero-anterior chest roentgenograms were taken for all the patients to evaluate any abnormal lesion in the chest. Sputum examination The sputum samples of the patients were collected in sterile plastic screw-capped containers. The specimens were examined microscopically for Paragonimus eggs and also for acid fast bacilli (AFB) using the wet cover slip smears and Ziehl-Neelsen-stained smears, respectively. The Paragonimus eggs were then preserved in two parts, one portion in equal volume of 10% phosphate-buffered formalin for morphological study and another in equal volume of 70% ethanol for molecular characterization. Microenzyme-linked immunosorbant assay (ELISA) test The blood samples of all the patients were tested for Paragonimus immunoglobulin G antibodies by micro-ELISA using antigens prepared from adult P. heterotremus worms. [6] Optical density (OD) values higher than 0.300 were taken as positive. Examination of crabs A total of 20 fresh water crabs were collected from a "Zachughie" mountain stream near the Pfutsero town. After morphological examination, the crabs were extracted and then digested with artificial gastric juice, followed by differential filtration. [7] The filtrates were examined under a stereoscopic microscope for P. metacercariae . The isolated metacercariae were preserved in two separate vials containing 10% formol-saline and 70% ethanol for morphological and molecular characterization, respectively. Morphological and molecular characterization Morphological features of eggs from the patients and metacercariae from the crabs were examined microscopically. Molecular characterization of eggs and metacercariae was performed by DNA isolation, amplification of the ITS2 regions of the ribosomal DNA by polymerase chain reaction (PCR)-linked restriction length polymorphism method and sequencing. [8],[7] To be more precise, the primers used were 3S (forward, 5′-GGTACCGGTGGATCACTCGGCTCGTG-3′) [9] and A28 (reverse, 5′-GGGATCCTGGTTAGTTTCTTTTCCTCCGC-3′). [10] The PCR amplification was performed using 0.25µm of each primer and 2.5U of Taq polymerase (Invitrogen Corp., Carlsbad, CA, USA). The amplified products were extracted from agarose gels (Lonza, Rockland, ME, USA) and sequenced using the corresponding primers and the BigDye Terminator Cycle Sequencing kit (Applied Biosystems, Foster City, CA, USA) on an automated sequencer (ABI 310 Genetic Analyzer; Applied Biosystems). The amplified products (10µm) were also treated with 5U of the restriction enzyme Apa LI (New England Biolabs, Beverly, MA, USA) at 37°C for 1h. The amplicons with or without the enzymatic treatment were then separated by electrophoresis on 2% (w/v) agarose gels. Results A total of 14 patients who attended the TB centre with some respiratory symptoms were investigated. The major clinical manifestations presented by them are shown in [Table - 1]. Chronic productive cough was the most common of all the complaints followed by difficulty in breathing and recurrent haemoptysis. In three patients, the sputum smears showed AFB while Paragonimus eggs were all negative. In 11 patients who were negative for AFB, two patients discharged Paragonimus eggs in the sputum. These two patients and four other patients who were negative for Paragonimus egg and AFB were positive for antibodies against the Paragonimus antigen. One smear-positive TB patient was also seropositive against the Paragonimus antigen. In summary, seven out of the 14 patients were positive for antibodies against the Paragonimus antigen. The OD values of the seropositive cases varied from 0.34 to 1.53, with 0.82 on average. Two patients who were egg positive showed much higher OD values (1.53 and 1.36) than the egg negative but seropositive patients. Of the seven paragonimiasis cases, there were five male and two female, making a male-to-female ratio of 5:2. In addition, a higher prevalence of paragonimiasis was detected among children and young adults in the age group of between 7 and 32 years and rare after 40 years of age. The chest roentgenograms showed abnormal areas in three of the seven seropositive patients (paragonimiasis). Left-sided pleural effusions were seen in two patients whose sputa were Paragonimus egg positive and right lung pneumonia in another seropositive patient. Out of the three TB patients, no abnormal lesions were detected in two while nodular shadows were seen in the right upper lung in one. This patient was infected with both Paragonimus (seropositive) and TB. Fever, weakness, weight loss and loss of appetite were found as other associated symptoms in this patient. The morphological features of the eggs from the two patients [Figure 1a] were found to be characteristic of P. heterotremus with some variations in the shape and size. They were oval and elongated in shape, golden-yellow in colour and operculated and measured 82-95µm (average = 82µm) in length and 45-58µm (average = 49µm) in width. The eggshell thickness was almost uniform and indiscernible at the non-operculated end. The freshwater crabs captured in the stream near Pfutsero town were morphologically identified as Potamiscus manipurensis [Figure 1b]. Of the 20 freshwater crabs examined, 48 P. metacercariae were isolated. Five smaller crabs (carapace size: 20.5mm x 24.5mm on average) and 15 larger crabs (carapace size: 29mm x 37mm on average) yielded 30 and 18 metacercariae, respectively. The number of metacercariae per crab was higher in smaller crabs (average = 6) than in bigger crabs (average = 1.2). The fresh metacercariae [Figure 1c] were oval to suboval in shape, with a thin outer cyst wall and a thicker inner cyst wall, which was typically thickened at both poles, better defined in [Figure 1d]. The inner cyst measured on average 197µm in the long axis and 163µm in the transverse axis. The thickness of the inner wall was on average 6.4µm on the side and gradually thickened at the pole to 18.5µm on average. The oral sucker was smaller than the ventral sucker and was provided with a stylet. The morphological features of the metacercariae were characteristic of P. heterotremus . By PCR amplification, the ITS2 PCR products of about 520 bp were generated from the DNA samples prepared from the eggs from patients [[Figure - 2], lane 1] and metacercariae. Two fragments (about 350bp and 170bp, [Figure - 2]. lane 2) were generated from the PCR products (520bp) after digestion with a restriction enzyme Apa LI, which recognizes the sequences from P. heterotremus . [11] The PCR products were excised from agarose gels after electrophoresis and were used for sequence analysis. The analysis revealed that the aligned ITS2 regions were 461bp (without primer sequences) for both eggs and metacercariae. The obtained sequence data were deposited in the database GenBank/EMBL/DDBJ under accession numbers AB456558 and AB456559 for the metacercariae and eggs, respectively. They were the identical sequences. Similarity searches of the database revealed that the obtained sequences were identical to those from the metacercariae (AB308377) and eggs (AB308378) of P. heterotremus occurring in Manipur, India. [7] Discussion Although some occasional cases of paragonimiasis, which diagnosed initially as pulmonary TB, were already discovered in Nagaland, the detailed information about the disease was not available. The senior author, therefore, visited the health centre at Pfutsero in Nagaland to investigate further for paragonimiasis and Paragonimus during March 28-29, 2008. We determined the prevalence of paragonimiasis, and the egg detection rate of 14 patients who attended the health centre was 50% and 14%, respectively. The results of morphological and molecular characterization of Paragonimus eggs from sputum samples have established that P. heterotremus was the causative agent of paragonimiasis in Nagaland. This species has also been identified as a significant cause of human pulmonary paragonimiasis in Manipur and Arunachal Pradesh, India, [1],[2],[3],[4],[5] as well as in Southeast Asian countries like Thailand, Lao PDR and Vietnam. [12] We also determined the epidemiological factors responsible for infections with P. heterotremus . A high prevalence rate of 64% was observed in children and young adults (age ≤ 30). This finding was in agreement with that in Manipur in which two-thirds of the patients were in the age group of 11-30 years [2] and in Arunachal Pradesh in which the infection was higher (52%) in children (age ≤ 15). [13] Crabs are abundant in most of the mountain streams in the endemic areas in Nagaland. The villagers believed that raw crabs or its extract and soup provided them strength and nutrition. Some believed that ingestion of raw crab extract can cure fever and allergy. These activities are important modes of infection for local people, especially for the young adults. Therefore, it is imperative to undertake health educational programs for the prevention of paragonimiasis in this endemic area. General physical conditions of paragonimiasis were relatively good. The patients were quite ambulatory and apparently healthy looking. The symptoms were exacerbated just by hard physical activities, which often initiated bouts of haemoptysis. Generally, clinical symptoms and radiological appearances of paragonimiasis were overlapping with pulmonary TB thus resulting in an overdiagnosis of the non-tubercular cases as smear-negative pulmonary TB. Therefore, a detailed clinical history of illness, including dietary habit of consumption of crabs and laboratory investigation such as sputum examinations for Paragonimus eggs and serodiagnoisis, are essentially important in all cases with respiratory symptoms to avoid misdiagnosis. Once diagnosed as paragonimiasis, the disease can be effectively treated with praziquantel. Conclusion The result of this investigation revealed the first recognized endemic area of paragonimiasis in Nagaland. Fifty per cent of the patients who were attending the TB clinic with some respiratory symptoms were found to be suffering from pulmonary paragonimiasis based on a serological micro-ELISA test. Two patients who presented with bloody sputum showed Paragonimus eggs in the sputum smears. The infection was common in children and young adults up to 30 years. The chest roentgenograms were normal except in four of the seven seropositive patients. The clinical and radiological features of pulmonary paragonimiasis and TB are similar and, therefore, it should be emphasized that serodiagnosis and sputum examination for Paragonimus eggs are essential before concluding a case as smear-negative pulmonary TB.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09038t1.jpg] [mb09038f2.jpg] [mb09038f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}