 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
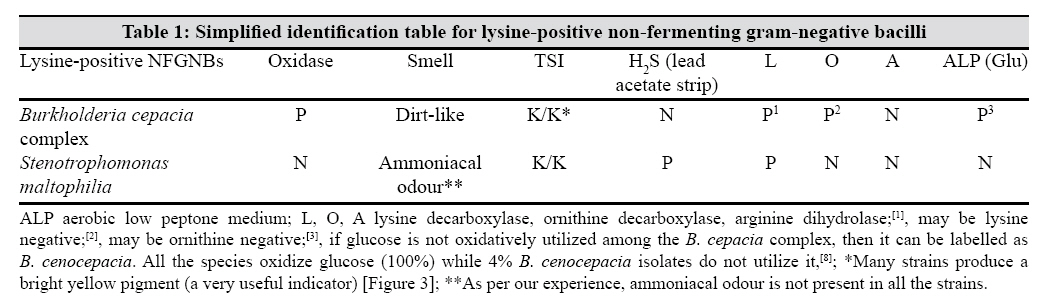
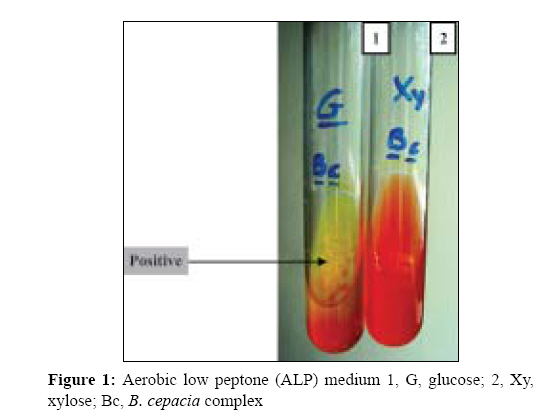
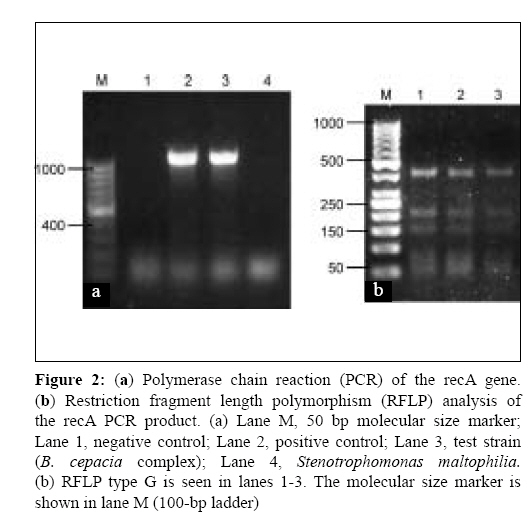
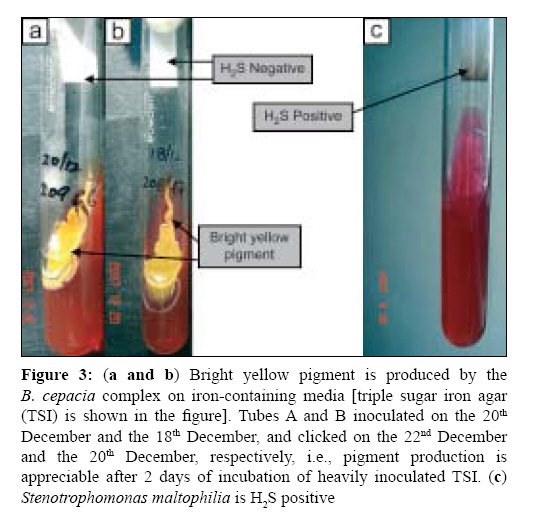
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 128-133 Original Article Identification of lysine positive non-fermenting gram negative bacilli (Stenotrophomonas maltophilia and Burkholderia cepacia complex) Gautam V, Ray P, Vandamme P, Chatterjee SS, Das A, Sharma K, Rana S, Garg RK, Madhup SK, Mahajan M, Sharma M Department of Medical Microbiology, Postgraduate Institute of Medical Education and Research (PGIMER), Chandigarh-160 012 Date of Submission: 26-Aug-2008 Code Number: mb09039 PMID: 19384035 DOI: 10.4103/0255-0857.49425 Abstract Background: The Burkholderia cepacia complex (BCC) and Stenotrophomonas maltophilia are closely related groups of non-fermenting gram-negative bacilli (NFGNBs) having a similar spectrum of infections ranging from superficial to deep-seated and disseminated infections. Identification of these lysine decarboxylase-positive NFGNBs lags behind in most Indian laboratories. A simplified identification scheme was devised for these two pathogens that allowed us to isolate them with an increasing frequency at our tertiary care institute.Materials and Methods: A simple five-tube conventional biochemical identification of these bacteria has been standardized. In the beginning, some of the isolates were confirmed from the International B. cepacia Working group, Belgium. Molecular identification and typing using recA polymerase chain reaction-restriction fragment length polymorphism was also standardized for BCC. For short-term preservation of BCC, an innovative method of preserving the bacteria in Robertson's cooked medium tubes kept in a domestic refrigerator was developed. Results: Thirty-nine isolates of BCC isolates were obtained from various specimens (30 from blood cultures) and 22 S. maltophilia (13 blood cultures and 9 respiratory isolates) were isolated during the year 2007 alone. Conclusions: BCC and S. maltophilia can be identified with relative ease using a small battery of biochemical reactions. Use of simplified methods will allow greater recognition of their pathogenic potential and correct antimicrobials should be advised in other clinical laboratories and hospitals. Keywords: Burkholderia cepacia complex , identification, India, stenotrophomonas maltophilia Introduction The Burkholderia cepacia complex (BCC) and Stenotrophomonas maltophilia are a closely related group of non-fermenting gram-negative bacilli (NFGNBs) found in many niches of both natural and clinical environments. Both have a similar spectrum of infections ranging from superficial to deep-seated and disseminated infections. BCC, a devastating pulmonary pathogen in cystic fibrosis (CF) patients, has also been reported as a cause of pneumonia, peritonitis and septicemia in non-CF patients. [1],[2] Its classification has undergone considerable taxonomic changes over the last two decades. The group is now known to encompass at least 10 distinct well-known species and five other novel species, whose laboratory identification can often prove difficult.[3] BCC has emerged as an important cause of morbidity and mortality in hospitalized patients largely because of the high intrinsic antibiotic resistance. BCC survives and multiplies in aqueous hospital environments where it may persist for long periods. [1],[4] Outbreaks of BCC septicaemia have been documented worldwide in intensive care units (ICUs), oncology units and renal failure patients. [5],[6] The incidence of disease due to these NFGNBs seems to be increasing. S. maltophilia is the third most common pathogenic NFGNB worldwide after Pseudomonas aeruginosa and Acinetobacter calcoaceticus-baumannii complex. [7],[8] BCC and S. maltophilia are exclusive members of the medically important lysine decarboxylase-positive NFGNB group (henceforth mentioned as lysine-positive NFGNBs). [7] It has always been a tedious task for a routine microbiological laboratory to identify the NFGNBs and poor laboratory proficiency in identification of these NFGNBs prevails worldwide, including in our own country. For this reason, reports of disease due to these organisms are rare from India. [2] Identification through commercial kits and automated systems is not fool-proof as many non- Burkholderia betaproteobacteria ( Ralstonia picketti and Pandoraea species) are labelled as BCC and some BCC strains as Pseudomonas aeruginosa. [9] Inherent in these lysine-positive NFGNBs is a contrasting susceptibility pattern to that of P. aeruginosa . These pathogens are among the most antimicrobial-resistant bacteria. BCC is intrinsically resistant to aminoglycosides and polymyxins and often develops resistance to β-lactams due to the presence of inducible chromosomal β-lactamases and altered penicillin-binding proteins.[8] Antibiotic efflux pumps in BCC mediate resistance to chloramphenicol, trimethoprim and fluoroquinolones. S. maltophilia is intrinsically resistant to most β-lactams, including carbapenems, the group commonly used in Pseudomonas infections. [8],[9] An upsurge of septicaemia due to NFGNBs was documented in our institute in 2004. Hence, we started identifying NFGNBs to the species level. About half of these (41%) strains in 2005 were lysine-positive BCC and S. maltophilia . We present the results of our investigation, some simple methods for identification and maintenance of these microorganisms and their antimicrobial susceptibility results. The most important area of our work is on BCC, which includes molecular identification and typing too. Therefore, more details are available for BCC below. The aim of this paper is to help routine diagnostic bacteriology laboratories to identify lysine-positive NFGNBs using only five tubes of conventional biochemical reactions with the available infrastructure and resources. Materials and Methods Bacterial isolates Bacterial culture was carried out in the clinical bacteriology laboratory of the Department of Medical Microbiology as a part of routine diagnostic services to the patients admitted in the hospital. The clinical isolates were identified by conventional biochemical tests. Gram-negative, motile, NFGNB were identified by the use of oxidase test, lead acetate paper strip for H 2 S production, lysine decarboxylase, ornithine decarboxylase and arginine dihydrolase and aerobic low peptone (ALP) medium slants (containing ammonium salts incorporated with glucose) [Table - 1]. Among BCC isolates, representative strains in the beginning were confirmed by the International B. cepacia Working Group at Belgium. BCC isolates were lyophilized and stored at 4°C for further reference. The identification of isolates as members of the BCC was confirmed by a triphasic analysis: 1. Conventional biochemical testing system [Table - 1] followed by 2. recA polymerase chain reaction (PCR)-based Identification. Molecular identification by PCR assays was based on the recA gene. [10] Three or four colonies of bacteria were taken from growth on nutrient agar plates and resuspended in Tris-ethylene diammine tetraacetate (EDTA) buffer. Genomic DNA was isolated using the Avegene system as per the protocol recommended by the supplier (Avegene, Taiwan). DNA was quantitated spectrophotometrically and approximately 20ng was incorporated into 25-mL reactions containing 1U Taq DNA polymerase, 250µM (each) deoxynucleoside triphosphate, 1.5µM MgCl 2 and 1X PCR buffer. Approximately 20 pmol of each appropriate oligonucleotide primer was added to each reaction and amplification was carried out using a thermal cycler for 30 cycles of 30 s at 94°C, 45 s at the appropriate annealing temperature and 60s at 72°C. A final extension of 10min at 72°C was applied to all thermal cycles. To avoid the non-specific bands, dimethylsulphoxide and formamide were added in concentrations of 0.25 µL/reaction and 0.32µL/reaction in the 25-µL reaction mix. PCR products were analysed by agarose gel electrophoresis (1.5%) using 1X Tris-EDTA buffer. Molecular size markers of the appropriate size range were included on all gels (100-bp DNA ladder). 3. Restriction fragment length polymorphism (RFLP) analysis for species identification. Species designation using RFLP of the recA PCR products further confirmed the identity of the strains. [10] To identify BCC isolates at the species level, RFLP analysis was performed. For RFLP analysis, 10µL of the PCR product was combined with the appropriate restriction enzyme buffer (5µL) and 1µL endonuclease (BsuRI) as outlined by the manufacturer (Fermentas, Canada) and incubated at 37°C for 1h. RFLP products were analysed by agarose gel electrophoresis (2.5%) using 1X Tris-EDTA buffer. Molecular size markers of the appropriate size range were included on all gels (100-bp DNA ladder or 1-kb DNA ladder; 50-bp ladder). [10] During the course of our experience, the medium base for oxidation-fermentation studies was changed from the classical Hugh and Leifson base to the ammonium phosphate-based ALP medium (Pickett, 1989). It was observed that acidification frequently occurred more quickly in the ALP medium [Figure - 1] than in the Hugh and Leifson sugars and no alkalinity that could mask the weakly acidic sugars, as can sometimes occur with Hugh and Leifson sugars, was observed. [11] Antimicrobial susceptibility Antimicrobial susceptibility testing was performed by the Kirby-Bauer disc diffusion method as per the Clinical Laboratory Standards Institute (CLSI), 2007 guidelines against co-trimoxazole, meropenem, ceftazidime, tetracycline and levofloxacin (control strains were Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853). [12] The piperacillin-tazobactam combination had also been tested. Minimum inhibitory concentration (MIC) For BCC isolates, MICs were performed by the agar and broth dilution methods against ceftazidime and tetracycline (control strains were Escherichia coli ATCC 25922 and Pseudomonas aeruginosa ATCC 27853). [12] Short-term maintenance of cultures Few colonies of BCC were passed in Robertson′s cooked meat medium (RCM) without paraffin and incubated at 35° C overnight. The RCM was then kept at 4° C. Isolates retained their viability for a minimum of 2 weeks. Preservation Brain heart infusion broth with 10% glycerol was used for preserving BCC. Two loopfuls (one can add more) of pure culture were added to vials containing 1mL of the stocking media and kept at −20° C. When reviving, the stock vials were kept at 37° C for half an hour and subcultured after overnight incubation in nutrient broth or peptone water onto a blood agar plate. If unsuccessful, the growth from the stock medium was inoculated into tryptone soy broth and then subcultured on to blood agar or MacConkey agar after overnight incubation. Lyophilization was performed as per textbook recommendations. [8] The chamber or batch method was used, skim milk was used as the cryopreservative and a very high initial inoculum of 10 10cfu/mL (recommended by Heckley) was used. The glass vials were stored at −20° C, as recommended. [8] While reconstituting, the vial surfaces were cleaned with 70% alcohol and both RCM broth and blood agar media were inoculated. A purity check was carried out for each isolate to rule out cross contamination. All reconstitution and preservation techniques were performed under sterile precautions in a Biosafety cabinet IIA. Results Of the 1235 positive blood cultures during 3 months (November 2004-January 2005), 170 (13.7%) were NFGNBs. Among these, 70 (41.2%) strains were identified as lysine-positive NFGNBs (BCC and S. maltophilia ) and others were identified as Alcaligenes spp. (40, 23.5%), P. aeruginosa (31, 18.2%) , Chryseobacterium indologenes (1, 0.6%) and Brevundimonas diminuta (1, 0.6%), respectively. Twenty-seven (16%) strains could not be identified by the limited available conventional biochemical tests. In 2005 (September-December), of the 7779 blood cultures, 74 (29.1%) lysine-positive NFGNBs were obtained out of 254 NFGNBs. In 2006-2007 (September-December) of the 8601 blood cultures, we isolated 25 (11.36%) lysine-positive NFGNBs among 220 NFGNBs. Lysine-positive NFGNBs were also isolated from respiratory samples (bronchoalveolar lavage and sputum). Thirty isolates of BCC and 20 of S. maltophilia were obtained in the year 2006. Thirty-nine isolates of the BCC were obtained from various specimens (30 from blood cultures) and 22 S. maltophilia (13 blood cultures and 9 respiratory isolates) isolates were isolated during the year 2007 alone. The results of the antimicrobial susceptibility testing by the disc diffusion method are given in [Table - 2]. By MIC testing, 80% BCC isolates (32/40) were sensitive to ceftazidime while 82.5% strains were resistant to tetracycline (33/40). Of the 41 isolates collected over the last 4 years and subjected to recA PCR-RFLP, 22 isolates were identified as B. cenocepacia IIIA (recA PCR-RFLP type G) [Figure - 2], two were identified as B. cenocepacia IIIB (recA PCR-RFLP typeAN) and seven were identified as B. cepacia (recA PCR-RFLP type E). In four isolates, no band was obtained and another four isolates revealed a faint band. A different base pair band was obtained in one isolate and one isolate among the five isolates of a single patient was lost. Discussion Identification of these organisms is tedious. We devised a simple algorithm for identification and preservation of these organisms in the laboratory. Over a span of 4 years, the number of biochemical reactions has been reduced from 16 to just five and substantiated by the molecular identification. Further, the identification period has been shortened to just 1 week from 1 month. With expertise, the identification can be performed the next day if biochemical reactions are properly inoculated. Further, one out of 10 known species (formerly, genomovar) of the genus Burkholderia can be labelled without molecular processing. However, on performing recA PCR, the isolates that do not yield a product of the right size, a double product, a faint product or a product with the wrong size are not considered BCC. Many laboratories are identifying the organisms by automated systems. However, when Burkholderia species are tentatively identified using an automated system, the identity of an isolate should be confirmed by conventional biochemical testing and, if necessary, molecular techniques. [8],[13] We have encountered cases where S. maltophilia has been labelled as BCC (95% probability indicated by the system) and another system labelled BCC as B. pseudomallei (99% probability) . One limitation of these conventional methods is that we are likely to miss lysine-negative BCC. Thirty BCC isolates were identified by conventional methods in the year 2006 from blood cultures and 39 isolates of BCC isolates were obtained in the year 2007 from various specimens. In comparison, a study by Reik et al. isolated only 90 strains over a span of 8 years from various clinical specimens of non-CF patients. [14] Of the 41 isolates collected over the last 4 years and subjected to recA PCR-RFLP, 31 isolates were identified as BCC. In four isolates, no band was obtained and another four isolates revealed a faint band. Although a faint band is taken as negative, in our experience, in one such strain, the RFLP pattern type G was obtained ( B. cenocepacia , RFLP type IIIA). In one strain we obtained a sharp non-specific band and one isolate was lost. However, the sensitivities and specificities of such PCR assays for the intended target species are difficult to determine in the absence of a reliable "gold standard". [8] Unidentified isolates have been present in previous epidemiological studies, [15] and it seems likely that the number of genospecies constituting the BCC complex may continue to rise. [3] In a recent Brazilian study also, 41 CF isolates of BCC were identified by culture and confirmation of identity and genomovar determination was obtained in 32 isolates by recA PCR. [15] B. cenocepacia (earlier genomovar III) is further divided into at least four phylogenetic lineages (IIIA, IIIB, IIIC and IIID). [16] Of the 41 isolates subjected to recA PCR-RFLP, 22 isolates were identified as B. cenocepacia IIIA (recA PCR-RFLP type G) [Figure - 2]. The importance of molecular identification lies in the fact that certain genomovars are associated with higher transmission and poor prognosis. [13] We have observed very little species-level diversity in our collection. This is an issue of concern that we have got the predominance of B. cenocepacia (genomovar IIIA; RFLP type G) that is associated with a high mortality rate. We have isolated this species from almost all the wards with predominance from ICU, paediatric ICU, paediatric emergency and bone marrow transplant units (data not shown), probably relating to its higher transmission rate. Because of the high intrinsic resistance of the BCC to antimicrobial compounds, these infections can prove very difficult to treat and may be fatal. [17] Often reported as Pseudomonas species, the value of proper identification comes to the forefront. The antimicrobial susceptibility profile of our isolates reveals near-complete resistance to aminoglycosides, fluoroquinolones and more than 50% resistance to carbapenems, the first-line therapeutics of choice against serious pseudomonal infections. These isolates behaved similar to non-CF nosocomial Italian isolates by showing susceptibility to ceftazidime. [18] As per the CLSI guidelines, the drugs recommended against BCC are ceftazidime, minocycline, meropenem and co-trimoxazole, and minocycline, levofloxacin and ceftazidime are recommended against S. maltophilia. [12] A microbiologist or trained technician can suspect these NFGNBs, noting the different colony morphology and odour (from P. aeruginosa ) on the first isolation. Then he/she can put up the sensitivity against five of the common drugs for these lysine-positive NFGNBs on a single sensitivity plate. Although a ubiquitous organism, isolates of BCC do not survive long on culture plates. The BCC grows well on most laboratory media but may lose viability on blood agar in 3-4 days. [19] Maintenance in RCM is very useful for early and easy revival of these organisms. These organisms survived for a minimum of 14 days, which helped us in working with them. The RCM preservation method is yet to be standardized in a proper manner as performed for Vibrio cholerae isolates. [20] One can inoculate the strain in RCM and carry on the identification as decarboxylases have to be kept for 5-7 days before reporting as negative. However, the decarboxylases give a positive result by the next day if minor modifications are made. Inoculate with a heavy inoculum of 0.5mL of the decarboxylase medium (properly adjusted pH) and then add liquid paraffin to it. In addition, a bright yellow pigment is produced by the BCC on iron-containing media (like triple sugar iron agar, heavily inoculated), which becomes more prominent after 2-3 days of incubation. The BCC does not survive in nutrient stab agars. If we need to transport these organisms, it can be carried out on nutrient agar slants. We have already tested our 10% brain heart infusion-glycerol broths stored at −20° C (−80° C is better) and lyophilized ampoules (best method of preservation) to find these organisms viable after 4 years (longer period revival is yet to be carried out). Lyophilization technique is considered the gold standard for long-term preservation of bacteria and fungi. [8] The technique retains its extreme usefulness even in gram-negative bacteria like the NFGNBs, in spite of a slight fall in viability. It can be concluded that BCC and S. maltophilia can be identified with relative ease using a small battery of biochemical reactions. Use of simplified methods will allow greater recognition of their pathogenic potential and correct antimicrobial advice in other clinical laboratories and hospitals.[Figure - 3] Acknowledgement The authors wish to thank Dr. Anand Desmukh, Qatar, Gulf (formerly Consultant Microbiologist, Breach Candy Hospital, Mumbai, India) for identifying the strains by the commercial identification system API 20NE (Biomerieux). We acknowledge the experience of Dr. Pradeep Singal, Genome Diagnostics, Delhi, for suggesting cosolvents (dimethylsulphoxide and formamide) to avoid non-specific bands in PCR. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09039f3.jpg] [mb09039t1.jpg] [mb09039f2.jpg] [mb09039t2.jpg] [mb09039f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}