 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
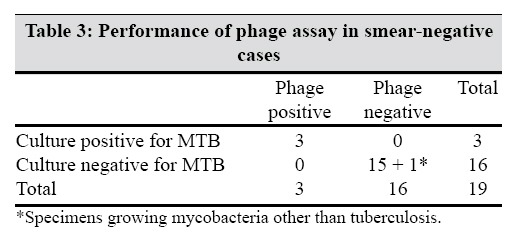
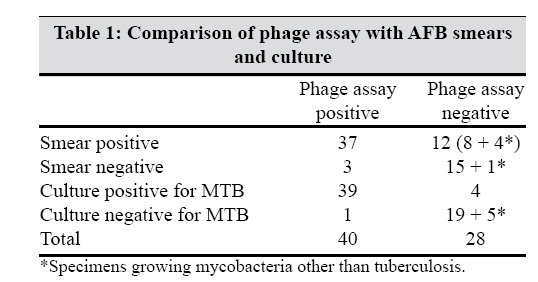
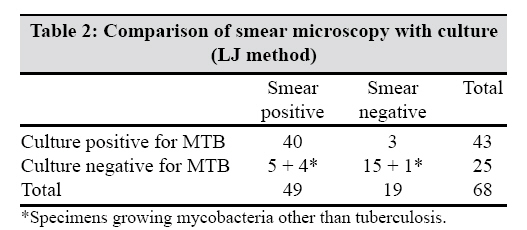
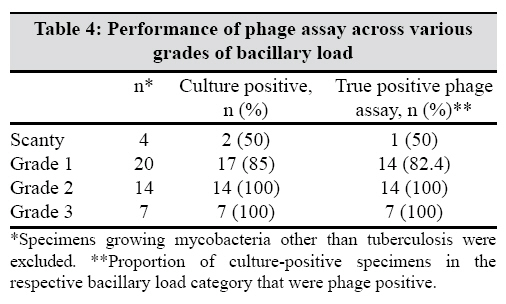
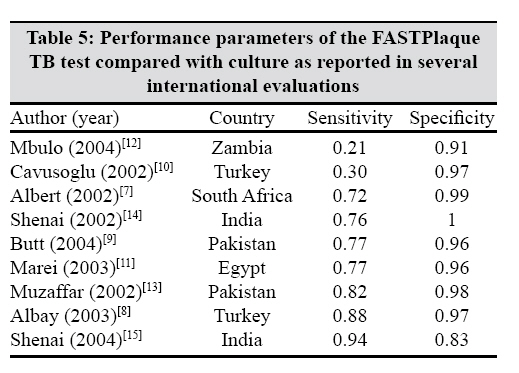
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 134-138 Original Article Clinical evaluation of the mycobacteriophage-based assay in rapid detection of Mycobacterium tuberculosis in respiratory specimens Prakash S, Katiyar SK, Purwar S, Singh JP Department of Tuberculosis and Respiratory Diseases, GSVM Medical College, Kanpur - 208 002 Date of Submission: 15-Oct-2008 Code Number: mb09040 PMID: 19384036 DOI: 10.4103/0255-0857.49426 Abstract Context: Search for a cost-effective, rapid and accurate test has renewed interest in mycobacteriophage as a tool in the diagnosis of tuberculosis (TB). There has been no reported data on the performance of phage assay in a high burden, low-resource setting like Kanpur city, India.Aims: To assess the sensitivity and specificity of the FASTPlaque TBTM kit ability to impact the bacillary load in the phage assay and its performance in the sputum smear sample negative cases. Materials and Methods: The study involved a cross-sectional blinded assessment of phage assay using the FASTPlaque TBTM kit on 68 suspected cases of pulmonary TB against sputum smear microscopy by Ziehl-Neilsen staining and culture by the LJ method. Results: The sensitivity, specificity and positive and negative predictive values of the phage assay were 90.7, 96, 97.5 and 85.7%, respectively. The assay was negative in all the five specimens growing mycobacteria other than TB. The sensitivity of the phage assay tended to decrease with the bacillary load. Of the smear-negative cases, three were false negative, and all of which were detected by the phage assay. Smear microscopy (three smears per patient) had a sensitivity and specificity of 93 and 64%, respectively. Conclusions: The phage assay has the potential clinical utility as a simple means of rapid and accurate detection of live Mycobacterium tuberculosis bacilli; however, its performance has been inconsistent across various studies, which highlights that the assay requires a high degree of quality control demanding infrastructure and its performance is vulnerable to common adversities observed in "out of research" practice settings like storage, transport and cross-contamination. Keywords: Diagnosis, mycobacteriophage, Mycobacterium tuberculosis, pulmonary Introduction India is classified along with the sub-Saharan African countries to be among those with a high burden and the least prospects of a favourable time trend of tuberculosis (TB) as of now, a problem that is further compounded by limited resources. [1] Recent estimates from the World Health Organization suggest the incidence of 168 cases/100,000/year and a prevalence of 299cases/100,000/year. [2] Smear microscopy is the mainstay in the diagnosis of TB under these settings. Although cheap, simple and quick, smear microscopy suffers from low specificity and variable sensitivity and can neither differentiate between live and dead bacilli nor identify mycobacteria other than tuberculosis (MOTT). The quality of results is heavily dependent on the workload, skill and motivation of the technician reading the slides and number of bacilli in the specimen and can be easily compromised in a high-volume, low-resourced laboratory. Smear microscopy alone can miss one-third to two-third of all cases of pulmonary TB who are infective and can transmit disease. [3],[4] Mycobacterium tuberculosis (MTB) culture is more sensitive. However, is time consuming and susceptible to contamination problems. [4] Availability of reliable labs performing good-quality culture is limited to some centres and inaccessible to the patient population at large. Rapid diagnosis of this disease is essential in view of its infectious nature, high burden of cases and emergence of drug resistance. The search for a cost-effective, rapid and accurate test has renewed interest in mycobacteriophage as a tool in diagnosis and drug susceptibility testing. FASTPlaque TB TM is a novel phage amplification technology that has been developed for rapid detection (within 48 hours) and enumeration of the MTB complex from clinical specimens. The results are read by the naked eye, are simple to interpret and need no specialized equipment. This method, which has been described later, uses specific mycobacteriophages to detect the presence of viable TB bacilli in the clinical specimen. [5],[6] There are studies on the performance of the phage assay, but there has been a great degree of variation in the reported data and, moreover, there have been none reported from a high-burden, low-resource setting like Kanpur city, India. Many studies have not reported the number of specimens growing MOTT, which can affect the results. Also, many studies have not reported on the patient population and human immunodeficiency virus (HIV) prevalence. Except a few studies, [7] in which the patients provided two sputum specimens each, all studies used only a single sputum specimen for smear microscopy. This approach differs from the current WHO and International Union Against Tuberculosis and Lung Disease recommendations, which state that at least three specimens must be examined for each patient. Use of a single specimen might make the smear microscopy look less sensitive. Considering these issues, we conducted a study to determine the clinical utility of phage assay against sputum smear microscopy in suspected cases of pulmonary TB at Dr. ML Chest Hospital, Kanpur. Materials and Methods The study comprised of a cross-sectional blinded analysis of sputum specimens collected from suspected cases of pulmonary TB attending the outpatient department of Dr. ML Chest Hospital, a tertiary-level government teaching hospital, affiliated to the GSVM Medical College, Kanpur, serving a large and diverse TB patient population from Kanpur and adjoining districts. The patient population was a mix of treatment naοve, previously treated and currently on treatment. Patients giving written consent were made to submit three sputum specimens - one spot on the first day and one early morning and one spot specimen on the second day. For each subject, three smears were examined by Ziehl-Neilsen (ZN) staining for acid fast bacilli (AFB) from the three specimens respectively. Pulmonary TB smear positive was defined as "at least two sputum smear positive out of three or one sputum positive out of three with positive culture report". The first spot specimen was sent for culture and phage test to separate blinded laboratories. Data recorded included age, sex, laboratory findings and past and current details of medication. Patients were subjected to voluntary counselling and testing for HIV (Microlisa-HIV, J. Mitra and Co. Pvt. Ltd., New Delhi, India) and the results were recorded ensuring patient anonymity. Institutional ethical clearance was obtained as a purely observational study. Decontamination and concentration of specimens All specimens were decontaminated by the standard N-acetyl-L-cysteine-NaOH method followed by centrifugation. The sediment was resuspended in 2 ml of sterile 0.67 M phosphate buffer (pH 6.8) and used for phage assay and cultures by the Lowenstein Jensen (LJ) method. FASTPlaque TB assay The assay was carried out using the FASTPlaque TBT kit, which included ActiphageT and VirusolT (Biotec Laboratories Ltd., Ipswich, UK). All specimens were processed according to the manufacturer′s instructions. Both positive and negative controls were also included. Negative control comprised of 1 ml of plain FASTPlaque TB broth. Three positive controls were prepared by serial dilution (10 2 , 10 -4 , 10 -6 ) of M . smegmatis . These controls were set up to assess the integrity of the phage and the effectiveness of the phagicidal agent. For the assay, 1 ml of decontaminated and concentrated sediment was mixed with 1 ml of FASTPlaque TB broth and incubated at 37°C overnight to enrich viable TB bacilli. Following enrichment, 100 µl of the mycobacteriophage solution (ActiphageT) was added and incubated for a further 1 hour for the infection to take place. Then, 100 µl of the virucide solution (VirusolT) was added and incubated at room temperature for 15 minutes for destruction of all bacteriophages that had not infected the host cells. Thereafter, 5 ml of FASTPlaque TB medium was added to neutralize excess virucide followed by 1 ml of helper cells (SensorT). After mixing thoroughly, it was added to the Petridish and overlayered with 5 ml of molten agar. On pouring, the plates were rotated several times and were allowed to set and were incubated at 37°C overnight. The number of plaques formed was counted. As recommended by the manufacturer, a cutoff of 20 plaques was used to interpret the results. LJ method Of the processed specimens, 0.5 ml was inoculated on two slants of LJ medium and incubated at 37°C. The slants were inspected every day for first week and then weekly for 10 weeks. All culture positives were confirmed by ZN microscopy and MOTT were detected by PNB and niacin test. Statistical analysis The dichotomous outcome variable of the investigations was cross-tabulated against each other. "Culture positive" was defined as culture growing the MTB complex and hence cultures growing MOTT were treated as "culture negative". The sensitivity, specificity, positive predictive value (PPV) and negative predictive value (NPV) for the phage assay were calculated against the AFB smear and the LJ slants. The association, if any, between phage assay results and sputum bacillary load grades was assessed using the χ2 test. Results The mean age of the subjects was 43 years. The number of males was 45 and females was 23. The number of HIV+ cases was two. The comparison of phage assay with AFB smear of sputum specimens is shown in [Table - 3]. Of the 49 sputum smear-positive specimens, 12 were phage negative, of which five were identified as MOTT, five were late culture positives and three were culture negative. The analysis of [Table - 1], which compares phage assay to smear microscopy, reveals sensitivity, specificity, PPV and NPV of 75.51, 84.21, 92.5 and 57.14%, respectively. Also shown is performance of the phage assay against culture. Four LJ-positive phage-negative specimens were late culture positives. Phage assay was negative in all the five specimens growing MOTT. The analysis of [Table - 1] for phage assay against culture, reveals sensitivity, specificity, PPV and NPV of 90.7, 96, 97.5 and 85.71%, respectively. [Table - 2] reveals performance of smear microscopy against culture, with sensitivity, specificity, PPV and NPV of 93, 64, 81.63 and 84.21%, respectively. Performance of phage test among sputum smear-negative patients is shown in [Table - 3]. There were no false-positive or false-negative phage results among the smear-negative cases. Of the 19 sputum smear-negative cases, there were three falsely negative smears, all of which were detected by the phage assay. Impact of bacillary load on phage assay is shown in [Table - 4]. The sensitivity of the phage assay to detect live tubercle bacilli decreased at very low bacillary load (smear grade 1 and scanty) (P < 0.01, χ2 test). Discussion Phage assay can render results much earlier than culture and has the ability to detect live bacilli. In our study, the results of microscopy were available within 2 hours whereas the culture took 4-8 weeks. The phage assay gave results within 2 days, a time span that has been consistent through the literature. [7],[8],[9],[10],[11],[12],[13],[14],[15] Of the 68 sputum specimens, 49 were smear positive for AFB and 43 were culture positive for the MTB complex. Of the 12 smear-positive phage-negative specimens, two were found to be culture negative most likely due to the presence of dead bacilli as these cases were on antitubercular treatment. This suggests that the assay may have a role as a tool to monitor the treatment success as it detects only viable bacilli. The phage assay was negative in all the five specimens of MOTT, which highlights the specificity of the test for the MTB complex. The sensitivity and specificity of the FASTPlaque TB test with respect to the culture were excellent. The high specificity gives a high degree of confidence that a positive FASTPlaque TB result is representative of active disease. The results are also in agreement with the results obtained from other studies, as shown in [Table - 5]. However, there is significant variation in the sensitivity data throughout the literature. The heterogeneity in the sensitivity data may be due to many factors that vary from setting to setting and include transport and the potential impact of environmental conditions on specimen viability. Mbulo et al , [12] pointed out that the main disadvantage of a phage-based test compared with a sputum smear microscopy is that specimens need to be transported to a specialist reference laboratory. The sensitivity of the phage assay was 72% when the specimens were processed immediately and tests were performed daily [7] compared with a sensitivity of 29% when the processing of the specimens was delayed and the assays were run twice a week [16] Hence, rapid processing of specimens and initiation of the phage assay is important. This point was well taken care of in our study but delays in an out-of-research clinical practice setting may significantly deteriorate the sensitivity of the test. Sodium hydroxide, used to decontaminate the specimens, may damage the bacilli and can reduce the sensitivity of phage-based assays while the use of more gentle decontamination techniques can reduce the specificity of the test by failing to prevent contamination from other microorganisms. Cross-contamination within the laboratory is an important and perhaps the most frequent cause of false-positive tests. The rate of false-positive phage assay (culture negative and phage positive/all phage positives) in our study was 2.5%, which compares favourably with other reported studies from similar settings. [13],[14] This could be due to cross-contamination, but the strain was not determined and traced. The occurrence of a false-positive phage test highlights the necessity of a high-quality lab that follows stringent quality control, a feature that is also a prerequisite for culture. Our study had two HIV seropositive cases, both of which were smear negative but culture positive. Of these, one had MOTT isolated from culture. The phage assay was positive in the patient infected with MTB while negative in the MOTT-infected patient. This represents the advantage of phage assay in TB-HIV coepidemics where the number of false-negative and scanty smear cases may be high. However, as shown in [Table - 4], the sensitivity decreased with the bacillary load. On the contrary, the phage assay was able to detect all culture-positive smear-negative cases. The discrepancy appears to be due to the small number of culture-positive smear-negative (three) and culture-positive scanty smear-positive (two) cases that are likely to introduce error. Analysis of a larger number of such specimens is necessary to test the robustness of the phage assay in these challenging settings. Comparing grade 1 smear specimens with grades 2 and 3 indicates that the bacillary load does have some impact on the performance of the phage assay. Even if the sensitivity remains above 50% in these challenging settings, the phage assay will have a useful clinical utility in the early diagnosis of smear-negative cases, given the rapid and specific diagnosis, thereby reducing the chances of transmission and morbidity. Specimens in our study were collected from patients reporting to a tertiary care centre. Such patients are more likely to have advanced disease with a large bacillary load. Selection bias could also have played a role in influencing the diagnostic properties of the phage assay. However, as shown in [Table - 4], the specimens with low bacillary load (scanty and grade 1) were as frequent as high bacillary load (grades 2 and 3). Our study involved the examination of three sputum smears from the three sputum specimens respectively per patient, but the phage assay was performed on only the first specimen. It may be argued that the comparison of the three smears versus one phage assay is not fair. The three repeated phage assays have significant cost implications. Besides, as of now, there are no guidelines for the repeated phage assay in practice like that for the sputum smear. However, it would be interesting to study the affect of repeated phage assay on its sensitivity and specificity. Our study suggests that when a patient′s phage test is negative, there is roughly a one in six probability that the patient has TB. A negative test, therefore, does not exclude TB in patients suspected to have TB. Also, they do not have substantially higher accuracy than sputum microscopy. In addition, phage-based assays are much more complicated and labour intensive than microscopy and thus cannot be performed in primary-care settings; they require a laboratory infrastructure similar to that required for performing cultures. Also, the fact that phage-based assays are more expensive than smear microscopy and need a trained microbiologist makes them less suitable in resource-poor settings and smear microscopy would continue to be the mainstay in management unless the phage assay is developed further to deliver consistently high sensitivity and specificity by being robust enough to withstand common adversities in the primary care setting. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09040t4.jpg] [mb09040t3.jpg] [mb09040t5.jpg] [mb09040t2.jpg] [mb09040t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}