 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
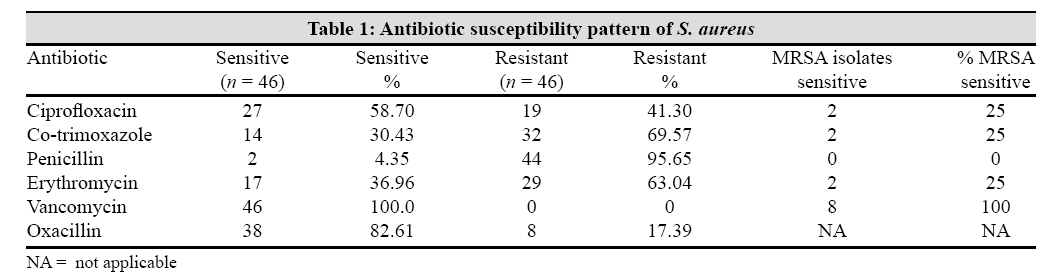
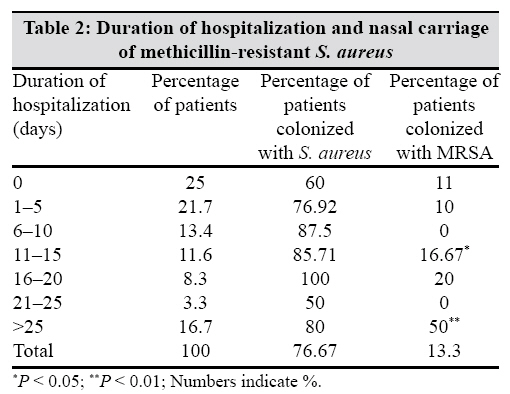
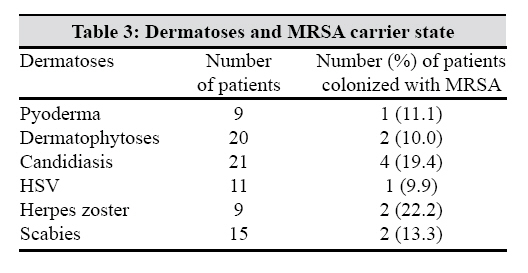
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 146-148 Brief Communication Factors affecting the nasal carriage of methicillin-resistant Staphylococcus aureus in human immunodeficiency virus-infected patients Chacko J, Kuruvila M, Bhat GK Department of Microbiology, Kasturba Medical College, Mangalore-575 001 Date of Submission: 12-Jul-2008 Code Number: mb09043 PMID: 19384039 DOI: 10.4103/0255-0857.49429 Abstract Human immunodeficiency virus-infected patients attending skin outpatient department were studied for nasal carriage of methicillin-resistant Staphylococcus aureus (MRSA) and associated factors affecting nasal colonization. Nasal swabs were used for isolation of S. aureus. MRSA were detected by agar screen and agar dilution methods. Careful examination for dermatoses was carried out. Forty-six of the 60 (76.67%) outpatients with HIV infection were colonized with S. aureus in the anterior nares. Significant number of S. aureus carriers were in the 31-40 year age group. Methicillin resistance was found in eight (17.39%) isolates. Of the 46 S. aureus strains, 29 (63%) were resistant to erythromycin, 69.5% to co-trimoxazole and 41.3% to ciprofloxacin. Co-trimoxazole use was found to be a risk factor for S. aureus carriage ( P = 0.0214) but not for methicillin resistance. Hospital stay for more than 10 days was a risk factor for methicillin resistance whereas stay for more than 25 days was found to be a highly significant risk factor. Dermatophytosis and herpes simplex virus infection were other risk factors for nasal carriage of S. aureus.Keywords: HIV infection, methicillin-resistant Staphylococcus aureus, nasal carriage The relationship between colonization with Staphylococcus aureus and human immunodeficiency virus (HIV) infection is of particular interest due to the morbidity and mortality associated with staphylococcal infections in these patients. HIV has been considered a known risk factor for colonization with S. aureus. [1],[2] Results of a previous study have shown that 31% of bacteraemias in HIV infections are caused by S. aureus . [3] Recent antibiotic use, CD4 T cell count < 200/ mm 3 , presence of central venous catheter, underlying dermatologic disease, broad spectrum antibiotic treatment and duration of hospital stay are considered to be the risk factors for methicillin resistant S. aureus (MRSA) colonization in HIV-infected patients. [4],[5] Varying prevalence of nasal carriage of S. aureus and MRSA among HIV-positive outpatients has been reported.[6],[7],[8] To the best of our knowledge, there are no reports on the carriage rates of S. aureus in HIV patients from this part of the country. There is also a lack of knowledge on the factors predisposing to nasal carriage of MRSA in HIV-positive patients. In a study by Nguyen et al. , [6] 34% were nasal carriers and carriage was significantly more common in patients with dermatologic conditions and those not receiving co-trimoxazole prophylaxis. In a study among drug users, 24% patients had positive S. aureus nasal cultures. [4] MRSA was more frequent in HIV-positive individuals (14%) than in non-infected individuals (3%). A previous study in Taiwan showed that 30% were colonized by S. aureus , 24% being methicillin-sensitive S. aureus and 6% being MRSA. The objectives of the present study were to determine the rate of nasal carriage of S. aureus in HIV-infected persons with special reference to MRSA and to determine the factors affecting MRSA colonization. Materials and Methods Sixty patients with HIV infection, attending the skin OPD at KMC Hospital, Attavar, Mangalore, were enrolled for the study after obtaining informed consent. The records of the patients were carefully scrutinized and details regarding duration of HIV infection from time of diagnosis, number of hospital admissions, duration of admission, number of hospital visits, invasive procedures carried out in the recent past, most recent CD4 T cell count in the records, details of previous opportunistic infections and current medications were noted. A careful examination for dermatoses was performed. Sterile swabs were swirled in both the anterior nares and transported immediately to the laboratory for processing. The specimens were inoculated on blood agar and Mac Conkey′s agar and incubated at 37°C for 24h. The staphylococci were identified by standard methods. [9] An antimicrobial susceptibility test was performed using the modified Kirby Bauer disk diffusion method. S. aureus ATCC 25923 was used as a control. MRSA was detected by agar screen and agar dilution methods. [10] S. aureus strains that had a minimum inhibitory concentration (MIC) of oxacillin ≤2μg/mL were considered methicillin sensitive and those having an MIC ≥4μg/mL were considered MRSA. Data were analysed using the χ2 test for continuity and a P -value < 0.05 was considered significant. Results Of the 60 HIV-infected persons, 46 (76.67%) were colonized with S. aureus, seven with S. epidermidis and two with Diphtheroids. Five persons were not colonized. The antibiotic susceptibility pattern of S. aureus is presented in [Table - 1]. Of the 60 patients, 31 (51.67%) were in the age group of 30-39 years. The rate of methicillin resistance did not show any correlation with the age of the subject. Among these 60 patients, 42 were males and 18 were females. The duration of HIV infection after laboratory diagnosis ranged from less than a year in 31 cases to more than 5 years in five. The S. aureus carriage rate and the rate of methicillin resistance showed no relation to the duration of the disease. Of the 45 patients admitted. 37 (82.2%) were nasal carriers of S. aureus . The rate of colonization with S. aureus was much higher in those patients who had been previously hospitalized (82.2%) compared with those who had never been hospitalized (60%). However, the risk was not statistically significant. In the colonized individuals who had been admitted previously, the duration of hospitalization varied between 1 and 5 days in 13 (28.89%) to more than 1 month in six (13.33%). Hospitalization for more than 10 days was a risk factor for methicillin resistance ( P = 0.0478) while admission for more than 25 days was found to be highly significant ( P = 0.0074) [Table - 2]. The number of hospital visits did not show any relationship with staphylococcal carriage or methicillin resistance. None of the invasive procedures independently or as a group were found to have a significant association with either S. aureus carriage or methicillin resistance. The rate of carriage was much higher in those patients who had received injections. The CD4 T cell counts ranged between 6 and 562/mm 3 . S. aureus carriage rates were higher (83.3%) in those patients with CD4 T cell counts < 200/mm 3 . No MRSA was found in patients with CD4 T cell counts more than 300/mm 3 . Of the 60 cases studied, 31 (51.66%) had tuberculosis, 11 (18.33%) had pneumocystis pneumonia and nine (15%) had cryptosporidiosis. Both the carriage rates and the methicillin resistance were higher in patients with systemic infections but it was not statistically significant. Among current medications, 31 (51.67%) were on antituberculosis drugs, 47 (78.33%) on antiretroviral treatment and 29 (48.33%) on co-trimoxazole. Of the 29 patients who received co-trimoxazole, 26 (89.66%) were colonized with S. aureus and this relationship was significant. The use of quinolones was closely associated with MRSA with high resistance rates (50%), but this was not statistically significant. Among the dermatoses present during examination, candidiasis was the most common, followed by dermatophytoses, scabies and herpes simplex virus infection. MRSA colonization was more common in patients with herpes zoster and candidiasis [Table - 3]. However, this relationship was not statistically significant. Discussion In the present study, a majority of the patients were males in the 30-39 years age group. This could be due to the fact that there are more males attending the HIV clinic in this hospital. Admission to hospital was not a risk factor for carriage of S. aureus and MRSA. Duration of hospitalization was a risk factor for colonization with MRSA. Administration of multiple drugs modifying the nasal flora could be a factor contributing to colonization of MRSA in this group. The rate of colonization with S. aureus and MRSA in the present study was higher compared with the study by Weinke et al. [1] The rate of MRSA was comparable with the study by Miller et al. [4] in a group of HIV-positive drug users (14%) and the study by Hidron et al. [10] (17%) where hospital-admitted patients constituted the study group. CD4 T cell count was not implicated in methicillin resistance. Similar findings have been reported by previous workers. [6],[11] A previous study showed that ciprofloxacin use could be an independent risk factor for S. aureus colonization. [7] The relationship between co-trimoxazole usage and nasal carriage was significant in this study. The rate of S. aureus nasal carriage varies according to the population studied. In the general population, a mean carriage rate of 37.2% has been reported. [12] Insulin-dependent diabetes mellitus, haemodialysis, intravenous drug addiction, skin infection and HIV infection are reported to be the risk factors enhancing the rate of staphylococcal carriage. Underlying dermatologic disease has been identified as a risk factor for MRSA. Among the dermatoses, dermatophytoses and herpes simplex virus infection were found to be risk factors for nasal carriage with S. aureus . However, no such association was found between MRSA and dermatoses. In the present study, S. aureus was more or less resistant to multiple antibiotics. This suggests that the bacteria could have been acquired during hospital stay or visit. In view of the serious morbidity and mortality that can occur with S. aureus infection, the high carriage rate in HIV-infected persons may require early intervention. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09043t3.jpg] [mb09043t2.jpg] [mb09043t1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}