 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 153-155 Brief Communication Leptospirosis outbreak in 2005: L.T.M.G. hospital experience Mathur Meenakshi, De Anuradha, Turbadkar Dilip Department of Microbiology, LTM Medical College and General Hospital, Sion, Mumbai-400 022 Date of Submission: 25-Feb-2007 Code Number: mb09045 PMID: 19384041 DOI: 10.4103/0255-0857.49431 Abstract Nine hundred and forty two serum samples from clinically suspected cases of leptospirosis admitted in Lokmanya Tilak Municipal General Hospital, Mumbai during July-September 2005 were tested by LeptoTek Dri-dot/Leptocheck. One hundred and sixty five positive sera by these tests were sent to I.R.R., Mumbai, for detection of leptospira IgM antibodies by ELISA (PanBio). Eighty seven positive sera were also sent to B.J. Medical College, Pune, for microscopic agglutination test (MAT) for serovar identification. Seropositivity with LeptoTek Dri-dot/Leptocheck was 34.3%. Adults and males predominated. All patients were febrile. The commonest presentation in adults was jaundice (81.4%), followed by oliguria (37.6%). In children, myalgia was commonest (75.6%), followed by conjunctival suffusion (54.7%). IgM ELISA positivity was 69.1% and MAT positivity was 29.9%. Commonest serovar detected in this geographical area was Leptospira icterohaemorrhagiae (42.9%), followed by L. bataviae, L. tarassovi, and L. pomona . Considering at least two of the above three serological tests positive, 127 cases could be diagnosed and only 89.8% of them could be diagnosed by ELISA and rapid test. Therefore, along with rapid serological tests, IgM ELISA should be routinely done for laboratory diagnosis of leptospirosis.Keywords: Leptospirosis, IgM ELISA, rapid tests, outbreak Leptospirosis is a febrile zoonosis of worldwide distribution. [1] Traditionally considered an occupational risk among persons exposed to contaminated water or infected animal urine, it is becoming recognized as a major public health problem, particularly in the tropics. [2],[3] In tropical and subtropical regions, the disease is endemic and exposure is widespread. [1] Clinical recognition of leptospirosis is difficult, due to its multisystem involvement. It presents with varied clinical manifestations and is often misdiagnosed as influenza, aseptic meningitis, encephalitis, dengue fever, hepatitis, or gastroenteritis. [3] Also, epidemics associated with high case fatality (>15%) break out annually during seasonal periods of heavy rainfall in areas that lack basic sanitation infrastructure. [2] Therefore, an accurate and rapid diagnosis of leptospirosis is essential, so that prompt specific treatment can be instituted as early as possible, to ensure a favorable clinical outcome. Similarly, quick and reliable typing of isolates is important to gain insight into the epidemiology and to design effective control measures. The sensitivity of blood cultures is low and culture isolation requires special media and up to six weeks of incubation. The microscopic agglutination test (MAT) is time consuming, requires technical expertise, and maintenance of multiple live serovars. [3] In response to this, various screening tests have been developed. The U.S. Food and Drugs Administration (FDA) has approved two assays - the indirect hemagglutination assay (IHA) and the immunoglobulin M (IgM) enzyme linked immunosorbent assay (ELISA) - for commercial use. [3] The city of Mumbai experienced heavy rains (944mm in 24 hours) on 26 th July, 2005, following which there was flooding and water-logging in the city. We report our experience of the postmonsoon deluge of 2005. Materials and Methods Nine hundred and forty two serum samples were obtained from clinically suspected cases of leptospirosis, admitted to L.T.M.G. Hospital during July-September 2005. All patients suffering from fever, and associated with at least one of the following sets of signs and symptoms as laid down by Indian Leptispirosis Society were included in this study: [4]
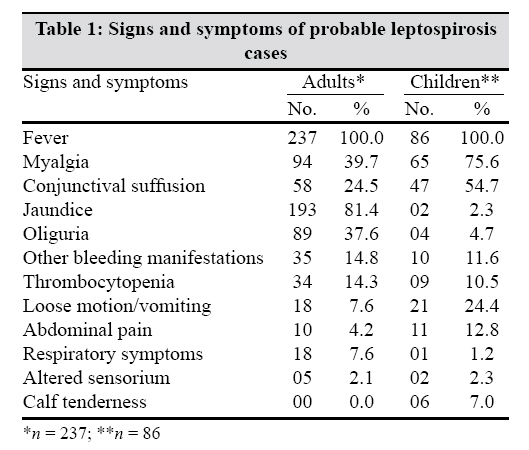
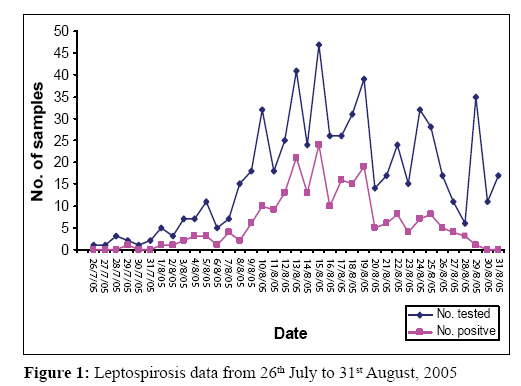
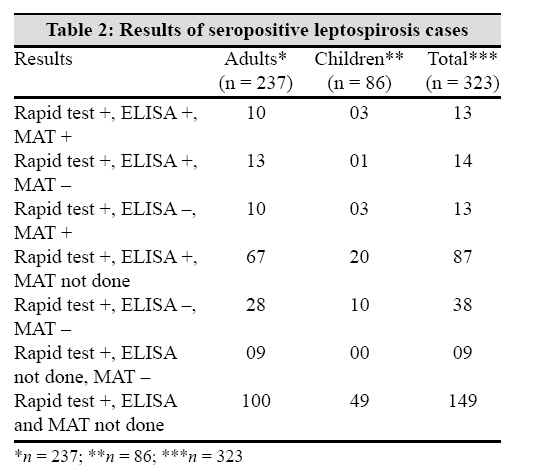
Rapid tests used were LeptoTek Dri-dot bioMerieux (Marcy l′Etoile, France) on 742 serum samples and Leptocheck WB Zephyr Biomedicals (Goa, India) on 200 serum samples. One hundred and sixty five sera positive samples by rapid test were sent to the Institute of Research and Reproduction (IRR), Mumbai, for detection of Leptospira IgM antibodies by ELISA. The kit used was PanBio (Brisbane, Australia) Leptospira IgM ELISA. Serum samples from 87 patients were sent to B. J. Medical College, Pune, for confirmation of serovars by MAT. Serovars included in the MAT panel were Leptospira icterohaemorrhagiae , L. tarassovi , L. canicola , L. bataviae , and L. pomona . Results Out of 942 serum samples, 323 were positive by LeptoTek Dri-dot/Leptocheck, with an overall seropositivity of 34.3%. This comprised of 73.4% adults (176 males and 61 females) and 26.6% children (61 boys and 25 girls). The adults to children ratio was 2.76 : 1 and males to females ratio was 2.76 : 1. The signs and symptoms of probable cases of leptospirosis are shown in [Table - 1]. The monsoon deluge was on 26 th July, 2005. First case of Lepto Dri-dot positive was reported on 29 th July, 2005, but this patient had no history of wading through waters. Practically, the first case of the outbreak was reported on 1 st August, 2005, that is, exactly six days after the deluge. Peak of positive LeptoTek Dri-dot cases was from 10-19 August, 2005 [Figure - 1]. After that, though the number of samples processed was more, the positivity of the leptospirosis cases gradually decreased as evidenced by the line graph [Figure - 1]. All the patients presented with fever. While jaundice was the predominant presentation in adults (81.4%), followed by oliguria (37.6%), myalgia (75.6%) and conjunctival suffusion (54.7%) predominated in children. Calf tenderness was seen only in children (7%). Respiratory symptoms were more in adults as compared to children, whereas loose motion, vomiting, and abdominal pain were more in children than in adults [Table - 1]. IgM ELISA positivity was 69.1% (114 out of 165). Twenty six sera samples out of 87 were positive by MAT (29.9%). The various serovars identified were L. icterohaemorrhagiae (42.9%), L. bataviae (25.7%), L. tarassovi (27.7%), and L. pomona (5.7%). In 20 serum samples, only a single serovar was isolated and six serum samples showed mixed reaction - two serovars in three samples and three serovars in three samples were identified. [Table - 2] shows the results of three serological tests. Considering at least two of the three serological tests positive, 127 leptospirosis cases could be diagnosed [Table - 2]. Out of 127, adults comprised of 100 (78.7%) and children 27 (21.3%). The ratio of adults to children was 3.7: 1. Only 114 (89.8%) cases out of 127 could be diagnosed by ELISA and by rapid test. All these 127 cases presented with fever. Jaundice was present in 65.4% patients, followed by myalgia in 51.2%, conjunctival suffusion in 32.3%, oliguria in 24.4%, and other bleeding manifestations (hemoptysis, hematemesis, hematuria, etc.) in 16.5%. Reduced platelet count was seen in 8.7% patients. Loose motion and vomiting was present in 11% and abdominal pain in 5.5% patients. Eleven patients (8.7%) presented with cough and breathlessness and only four (3.1%) had altered sensorium. Discussion Improved diagnostic tests for leptospirosis are urgently needed to help in the clinical diagnosis during the initial phase of the disease and for the rapid case confirmation during outbreak surveillance. Doxycycline therapy initiated soon after the onset of symptoms can prevent severe complications and mortality. [5] Though MAT is a widely used reference test it has its limitations as mentioned earlier. Moreover, MAT is inadequate for rapid case identification, as it requires analysis of paired sera and can only be performed in few reference laboratories. [2] Jeyakumar et al. , had reported an overall MAT positivity of 46.7%. [6] In this study, MAT positivity was only 29.9%. The low percentage can be explained by the unavailability of paired serum samples and that most of the samples were collected during acute stage of the disease. In the early stage of disease, MAT might give negative results or low titers (1 : 20). All sera positive by MAT in this study had titers of ≥1 : 150. The prevalent serovars in a particular geographic area must be known, as it is quite cumbersome to test for all 200 serovars of L. interrogans . [7] Only five serovars were included in the MAT panel at B.J. Medical College, Pune. This is also another reason for less MAT positivity in this study, due to the use of restricted number of serovars for confirmation. Recently, several rapid assays have been developed that can be used for screening of acutely ill patients. [1],[2],[3] The sensitivity of these tests ranges from 88-100% and specificity from 95-99.8%. [1],[8],[9] Gupta et al. , have reported sensitivity of IHA to be 100% and specificity 94% as compared to MAT. [10] LeptoTek Dri-dot assay has shown an overall sensitivity of 90% and specificity of 92%. [8] Both LeptoTek Dri-dot and Leptocheck WB were comparable screening tests in this study, as 254 samples out of 742 were positive by the former test (34.2%) and 69 out of 200 were positive by the latter (34.5%). Rapid tests are simple, easy to perform, cheap, and also have inbuilt controls. Maskey et al. , have reported a 31.8% serpositivity by the rapid tests during the monsoon deluge in 2005 in Mumbai. [7] This study has seropositivity of 34.3% by the rapid tests and adult and male predominance. In this study, apart from fever, jaundice predominated in adults (81.4%) [Table - 1]. Jeyakumar et al , have also reported high incidence of jaundice (81.4%) in leptospiral infections in Chennai. [6] In a serological study of jaundiced patients in Kolkata, MAT positivity was 23.8%, [11] as compared to our MAT positivity of 29.9%. PanBio Leptospira IgM ELISA has a sensitivity of 100% and specificity of 95.9%. [9] Therefore, entire seropositive samples by rapid test were subjected to ELISA. Considering at least two of the above three tests positive, 127 cases of leptospirosis could be diagnosed in this study [Table - 2]. Predominant symptoms were jaundice (65.4%), apart from fever in 100%, and myalgia in 51.2% cases. Out of 127 diagnosed cases, only 114 could be diagnosed by ELISA and screening test (89.8%) [Table - 2]. Therefore, along with rapid serological tests, IgM ELISA should be routinely done for laboratory diagnosis of leptospirosis. Those seropositive by ELISA, should be sent to reference laboratory for MAT, so as to identify the serovars present in that geographical area for control of leptospirosis. As leptospirosis is endemic in Mumbai, a detailed study of other serovars is also required. Acknowledgement We acknowledge IRR, Mumbai, for doing IgM ELISA and B. J. Medical College, Pune, for performing MAT for serovar identification.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09045t1.jpg] [mb09045t2.jpg] [mb09045f1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}