 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
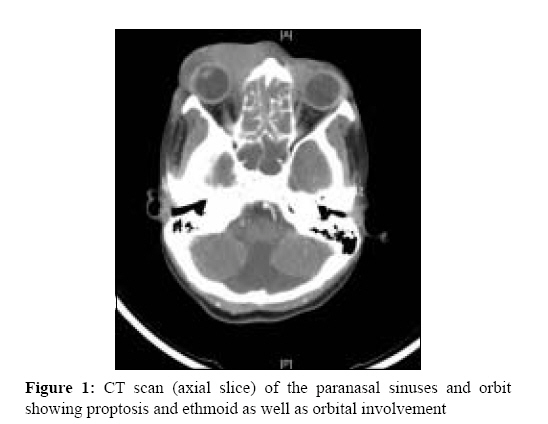
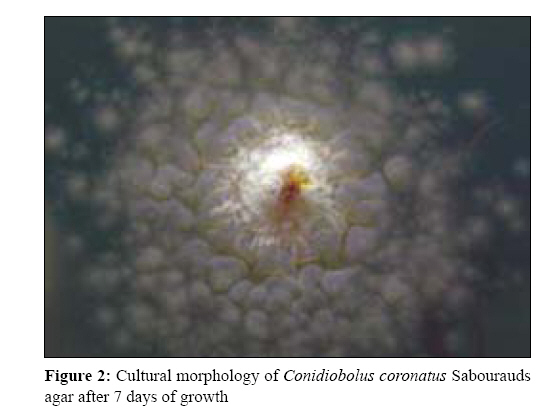
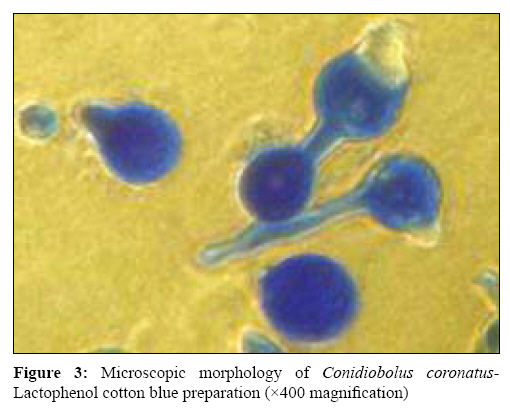
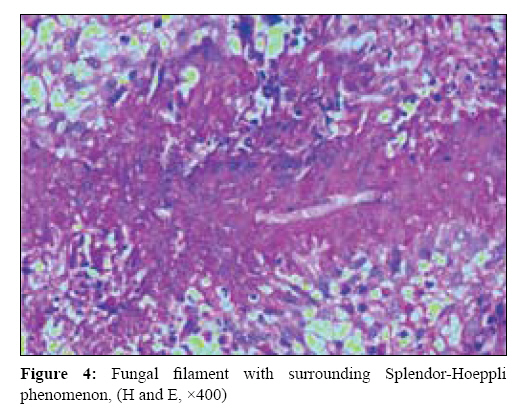
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 156-158 Case Report Unusual presentation of entomophthoromycosis Michael RC, Michael JS, Mathews MS, Rupa V Department of ENT, Christian Medical College, Vellore-632 004, Tamil Nadu Date of Submission: 17-Jun-2008 Code Number: mb09046 PMID: 19384042 DOI: 10.4103/0255-0857.49432 Abstract Rhinoentomophthoromycosis caused by Conidiobolus sp commonly presents as a chronic granulomatous lesion that affects the rhinofacial subcutaneous tissue. We present an 18-year-old girl who presented with progressive bilateral proptosis and loss of vision since 2 weeks. Biopsy and fungal cultures confirmed diagnosis of Conidiobolus sp infection of the paranasal sinuses bilaterally with orbital extension and blindness. The clinical picture was complicated by the presence of sputum-positive cavitatory pulmonary tuberculosis, which was diagnosed at the same time. To our knowledge, this is the first such case to be reported from India. We also discuss the management of entomophthoromycosis. Despite many reports of success, there remains no consensus on the treatment of Conidiobolus infections of the nose and the paranasal sinuses with antifungal agents.Keywords: Conidiobolus coronatus, rhinoentomophthoromycosis, zygomycosis Zygomycosis due to entomophthoraceous fungi is caused by the species of two genera, Basidiobolus and Conidiobolus . Rhinoentomophthoromycosis caused by Conidiobolus sp is a chronic, subcutaneous zygomycosis characterized by painless, woody swelling of the rhinofacial region. These fungi are ubiquitous in the environment and distributed in tropical areas, particularly in Central America, equatorial Africa and India. Most cases have been reported from India. [1],[2] Conidiobolus sp infections usually present as chronic inflammatory or granulomatous disease characterized by swelling of the nose, perinasal tissue and mouth. This is accompanied by symptoms of nasal obstruction, nasal drainage and paranasal sinus pain. The infection begins as a swelling of the inferior turbinates, with subsequent extension in the submucosa through the natural ostia to the paranasal sinuses and into the surrounding subcutaneous tissue. [3] There is generally no angioinvasion. [4] Affected individuals are usually immunocompetent although there have been reports of invasive forms of the disease in an immunocompromised host. In these cases, the organism behaves like an opportunistic pathogen. [5] We present a rare clinical presentation of entomophthoromycosis presenting as orbital cellulitis with blindness. This unusual presentation was also complicated by the fact that the patient had sputum-positive pulmonary tuberculosis, which was diagnosed at the same admission. Case Report An 18-year-old girl presented to the Ear, Nose and Throat (ENT) outpatient department in December 2007 with bilateral proptosis, periorbital swelling and progressive loss of vision in both eyes. She had intermittent low-grade fever for the last 15 days. She also complained of bilateral nasal obstruction and rhinorrhoea for the last 10 days. She had a history of contact with tuberculosis (her brother had pulmonary tuberculosis). Physical examination revealed an emaciated young girl with bilateral proptosis and preseptal cellulitis. There was bilateral periorbital and lid oedema with induration. Neck examination revealed palpable bilateral cervical lymph nodes. Ophthalmic examination revealed bilateral loss of perception to light and restriction of eye movements. Rigid nasal endoscopy showed bilateral mucopurulent nasal discharge with swollen inferior turbinates. No definite mass was seen. The rest of the ENT evaluation was normal. Blood investigation revealed a haemoglobin of 10.8mg%, total white cells of 15,300/mm 3 with 80% neutrophils and the erythrocyte sedimentation rate was 55mm at 60min. Liver and renal functions were normal. A computerised tomography (CT) scan of the paranasal sinuses and the neck [Figure - 1] with contrast showed a soft tissue mass with bilateral involvement of anterior and posterior ethmoids, nasal cavities and orbit. Orbital involvement was extraconal and the inferomedial and preseptal regions of the orbit were affected. Enhancing deep cervical lymph nodes were also present bilaterally. The chest X ray and CT scan revealed bilateral upper lobe consolidation with areas of cavitations. The patient was specifically evaluated with regard to her immune status and serology for hepatitis B surface antigen and human immunodeficiency virus, which were negative. Her blood sugar was within normal limits and there was no history of any immunosuppressant drug intake. These confirmed her immunocompetant status. The patient was started on broad spectrum intravenous antibiotics after the sputum culture results. She underwent an emergency endoscopic sinus surgery with debulking and biopsy of the lesion under general anaesthesia. Per operatively, a firm lesion that was partly vascular, partly granulomatous and partly polypoidal was found in both the middle meatus, the anterior ethmoids and the posterior ethmoids. There was no allergic mucin or fungal debris seen. Specimens were taken and sent for histopathology, bacterial and fungal cultures. The lung lesions seen on CT scans were investigated further. Three consecutive sputum samples sent for microbiological examination revealed the presence of numerous acid fast bacilli (AFB) on microscopy. The AFB cultures were positive for Mycobacterium tuberculosis after 4 weeks on Lowenstein-Jensen medium. The tissue received for fungal culture wasminced using sterile scissors. Direct microscopy of tissue with 10% potassium hydroxide and calcofluor white fluorescence stain was negative. Theminced tissue was cultured onto Sabourauds agar with and without antibacterial antibiotics. There was visible growth of colonies of Conidiobolus coronatus within 72 hours of inoculation of the specimen . The colonies grew rapidly and were flat, cream coloured and glabrous, which became radially folded and covered by a fine, powdery, white surface mycelium and conidiophores with satellite colonies around [Figure - 2]. Microscopic examination of the colony revealed spores that had a prominent broad projection at their site of former attachment to the sporangiophore [Figure - 3]. The primary spores germinated and produced sporangiophores, which further bore spores. Some of the primary spores had a corona formed by secondary spores. Histopathology of the biopsy showed granulomatous inflammation with fungal organisms consistent with zygomycosis. The fungal hyphae were surrounded by Splendor-Hoeppli phenomenon, as shown in [Figure - 4]. The patient was started on antituberculous treatment with Isoniazid, Rifampicin, Ethambutol and Pyrazinamide for a period of 2 months followed by Isoniazid and Rifampicin for 4 months. For the Conidiobolus infection, she was treated with oral Fluconazole 300 mg/day for 3 months. The patient was discharged with advice to review in the ENT outpatient department after 1 month of discharge from the hospital but was unfortunately lost to follow-up despite all attempts to trace her. Discussion The agents of entomophthoromycosis are normal inhabitants of the soil throughout the world. Although they are ubiquitous, the infection they cause is rare. Conidiobolus sp is found in soil and decaying vegetation, insects and in the gastrointestinal contents of lizards and toads. [6] The characteristic histopathological feature is the presence of large, aseptate or sparsely septate hyphae surrounded by eosinophilic hyaline material with subcutaneous granuloma. Deposition of eosinophilic material around microorganisms, called the Splendore-Hoeppli phenomenon, has been described not only in entomophthoromycosis but also in sporotrichosis, schistosomiasis and other infections. [6] There are two species of Conidiobolus that have been described to be pathogenic in humans, C. coronatus and C. incongruous . The colony morphology is similar but the microscopic morphology is slightly different. The former produces villose conidium and secondary conidia in addition to beaked conidia whereas the latter produces only beaked conidia and yellow zygospores. Paranasal sinus infection with C. coronatus usually begins with a unilateral involvement of the nasal mucosa and facial subcutaneous tissues, leading to the formation of firm, subcutaneous nodules or polyps. Most cases reported thus far have been non-invasive and dissemination is not common. Our patient had bilateral sinus involvement with proptosis and extensive invasion into the orbit. The patient probably acquired active pulmonary tuberculosis due to exposure to her family member with the disease. In addition, she was malnourished and from a low socioeconomic background, which favoured the spread of the disease. She had bilateral cervical lymphadenopathy, which was probably tuberculous lymphadenitis, as this condition is the most common form of extrapulmonary tuberculosis in young adult females in endemic countries. [7] To date, this is the first report of Conidiobolus and tuberculosis occurring together in an immunocompetent individual. A search on PubMed with the words "invasive entomophthoromycosis" and "coexisting tuberculosis" did not reveal any previous case reports. The treatment for entomophthoromycosis is both medical and surgical. Surgical debridement of the affected paranasal sinuses followed by systemic antifungal therapy is the treatment of choice. Treatment with antifungal drugs alone is, however, not always successful. Potassium iodide, co- trimoxazole, amphotericin-B, imidazoles and combinations of these agents have all been used with varying success. [4],[8] Recently, there have been reports of successful treatment with the azole group of antifungal agents. [9] We treated our patient with fluconazole. Long-term results with this have to be studied. These have been used either alone or in combination with other antifungal agents. In conclusion, we present an unusual case of a young girl with pulmonary tuberculosis and invasive subcutaneous rhinofacial infection caused by C. coronatus . Even though they are usually described as slow growing and cause subcutaneous mycosis, entomophthorales can cause acute invasive disease in immunocompetent individuals. This case is unusual in its presentation of two co-existent chronic granulomatous infections as well as the invasive and destructive nature of the Rhinofacial lesion caused by C. coronatus. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09046f1.jpg] [mb09046f2.jpg] [mb09046f4.jpg] [mb09046f3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}