 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
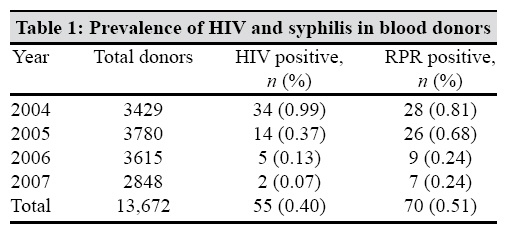
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 167-168 Correspondence Seroprevalence of human immunodeficiency virus and syphilis in blood donors of Delhi Ekadashi R, Langer S Delhi Heart and Lung Institute, 3 mm II Panchkuian Road, New Delhi-110 055 Date of Submission: 02-Jun-2008 Code Number: mb09051 PMID: 19384047 DOI: 10.4103/0255-0857.49437 Dear Editor, Transfusion of blood and blood products is a life saving measure that benefits numerous patients worldwide. At the same time it is an important mode of infection to the recipients. In up to 15% of the total patients infected with human immunodeficiency virus (HIV), blood transfusion has been the route of transmission. Syphilis positivity varies from 0.8% in voluntary donors to more than 15% in paid commercial donors. [1] Although HIV infection has been reported in all groups of blood donors in Delhi, it is particularly high among replacement donors. [2] Concealing the medical history by professional or replacement donors pose a great threat to safe blood supply. Problems are also due to the prevalence of asymptomatic carriers in the society, blood donations during the window period, genetic variability in the viral strains and laboratory errors. Only few reports are available regarding the trend of HIV seropositivity and syphilis serology, particularly in blood donors from northern India. [3] In this study, we aimed to assess the prevalence and trend of HIV and syphilis over 4 years, 2004-2007, among blood donors of Central Delhi. A total of 13,672 blood units were collected from blood donors during the period from January 1 2004 to December 31 2007 at the blood bank of Delhi Heart and Lung Institute in New Delhi, India. This is a tertiary care level hospital super specializing in heart and lung ailments. Blood donors were either replacement or voluntary. Care was taken to exclude professional donors by taking appropriate history and examination. All 13,672 serum samples were screened for HIV 1 and 2 and syphilis reactivity. HIV was screened using a third generation enzyme-linked immunosorbant assay kit biokit Bioelisa (Werfen Group, Barcelona, Spain, HIV 1 + 2 rec) with reported sensitivity and specificity of 100% and 99.98%, respectively. Syphilis serology was tested using the rapid plasma reagin (RPR) card test from (Tulip Diagnostics, Goa, India). Because of several constraints, positive cases of syphilis serology could not be confirmed using TPHA, which could have probably led to the avoidance of false positives. Of the total 13,672 blood donors, 13,198 (96.53%) were replacement and 474 (3.46%) were voluntary donors. More than 90% of the donors were males in the age group of 20-45 years. A total of 55 blood donors (0.40%) were seropositive for HIV infection ranging between 0.07% and 0.99%, showing a peak in 2004 [Table - 1]. HIV seropositivity has ranged from 0.50% (2007) to 0.64% (2005) among replacement donors and from 0.33% (2005) to 0.49% (2004) among voluntary donors. The χ2 test was used to statistically analyse data. HIV seropositivity was found to be significantly higher in replacement donors ( P < 0.05). The syphilis seroreactivity varied from 0.3% (2006, 2007) to 0.82% (2004) among replacement donors and from 0.09% (2007) to 0.4% (2004, 2005) among voluntary donors during the study period. The seropositivity for syphilis was also significantly lower in voluntary donors than in replacement donors ( P < 0.001). The RPR reactivity showed a decreasing trend in both voluntary and replacement donors between years 2004 and 2007. The HIV seroprevalance among paid and voluntary blood donors in New Delhi increased from 0.10% and 0.01%, respectively, in 1991 [4,5] to 0.33% among blood donors in 1994. [6] However, in our study, the seropositivity for both HIV and syphilis has shown a declining trend over the study period. This is particularly possible considering the similar mode of transmission of both. This study documents that seropositivity for HIV and syphilis was significantly higher in replacement donors. Based on these results, we feel that to reduce the risk of these infections non-remunerated repeat voluntary blood donor services are needed. Extensive donor selection and screening procedures can improve the blood safety. Emphasis must also be given on voluntary risk reductions, which will require increased awareness and change in attitude of people. Voluntary blood donations have to be made a part of a healthy lifestyle. Enlightening people about the benefits of voluntary blood donations and making it important for appraisals, admissions and employment can overcome this problem. All this, however, requires strong political commitment and multisectorial engagement. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09051t1.jpg] |
| |||||||||
{kind=link}