 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
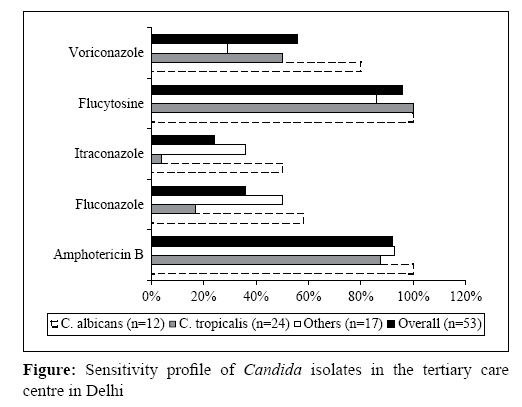
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 171-172 Correspondence Epidemiology of candida bloodstream infections in a tertiary care institute in India Kothari A, Sagar V BL Kapur Memorial Hospital, Delhi -110 005 Date of Submission: 15-Jul-2008 Code Number: mb09054 PMID: 19384050 DOI: 10.4103/0255-0857.49440 Dear Editor, The frequency of invasive, opportunistic mycosis has increased significantly over the past two decades. [1] Candida species account for 8-10% of all nosocomial bloodstream infections. [1] A major concern with invasive candidiasis is its association with an excess attributable mortality rate of 10-49%. [2],[3] This is directly related to the increasing number of patients at risk of serious fungal infections, including patients undergoing blood and marrow transplantation, solid- organ transplantation, major gastrointestinal surgery, patients with acquired immunodeficiency syndrome, neoplasia, on immunosuppressive therapy and premature infants. Most of the studies on candidemias have been carried out in Western countries, and there is a paucity of data from India that would help to direct therapy in these patients. The aim of this study was to determine the epidemiology of bloodstream candidal infections and to calculate the mortality associated with candidemia from our 400-bedded tertiary care centre in India. This was a retrospective data analysis from July 2005 to November 2006. Data from all inpatient positive blood cultures were analysed to determine the incidence of Candida -associated bloodstream infections, species distribution of candidal isolates and susceptibility profile to commonly used antifungal agents. Identification was performed using API ID32C (bioMerieux, Marcy l′Etoile, France) and broth microdilution susceptibility was performed using API ATB Fungus 3 (bioMerieux SA) kits using the mini API (bioMerieux SA) platform. All resistant isolates were confirmed using E-test ® (AB Biodisk, Solna, Sweden). The minimum inhibitory concentration of < 1mg/L was taken as sensitive for amphotericin B, < 8mg/L for fluconazole, < 1mg/L for voriconazole, < 0.12mg/L for itraconazole and < 4mg/L for flucytosine. Mortality associated with candidal bloodstream infections was also determined. Candida spp. accounted for 18% of all nosocomial bloodstream infections in our institution. There were 53 episodes of candidemia detected in the 17-month period in 48 patients. Of these, 45% were caused by C. tropicalis , 23% by C. albicans and 32% by other Candida spp. The susceptibility profile of all candidal isolates showed that 92% were sensitive to amphotericin B, 36% to fluconazole, 24% to itraconazole, 56% to voriconazole and 96% to flucytosine. Notably, while all strains of C. albicans were susceptible to amphotericin B, 42% were resistant to fluconazole. C. tropicalis , the most commonly isolated species, was susceptible to amphotericin B in 87.5% of the isolates and to fluconazole in only 17% of the cases. Mortality associated with candidal bloodstream infections was 60% [Figure - 1]. While in western literature C. albicans is associated with 50-70% of all episodes of candidemia, [1] our data suggest that in the Indian setting C. tropicalis is the most common This is in line with earlier data from the Indian subcontinent, which showed that non-albicans Candida can cause from 67 to 90% of nosocomial candidemias and C. tropicalis was the most commonly isolated agent causing 36% of the cases. [4],[5] Western data have shown that the most common species of Candida , including C. albicans, C. parapsilosis and C. tropicalis remain reliably susceptible to the polyenes, flucytosine, azoles and echinocandins. [1] In India, while amphotericin B remains the drug of choice for empirical treatment of invasive candidiasis, azoles like fluconazole can no longer be used even for cases of C. albicans infection, as indicated by our data. Even voriconazole, which is the newest-generation azole available in India, shows an extremely high resistance of 56% to all Candida spp. This is an extremely disturbing trend, possibly associated with increased use of azoles as prophylaxis, especially in surgical units and intensive care units. Our study highlights the fact that epidemiology of invasive candidiasis in India differs markedly from that in Western countries. It is important to monitor resistance trends and distribution of Candida spp in the face of increasing usage of potent, broad-spectrum antibacterial agents in hospitals in India. We should develop local guidelines on treatment of invasive candidiasis based on the epidemiology of infection in the Indian subcontinent. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09054f1.jpg] |
| |||||||||
{kind=link}