 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
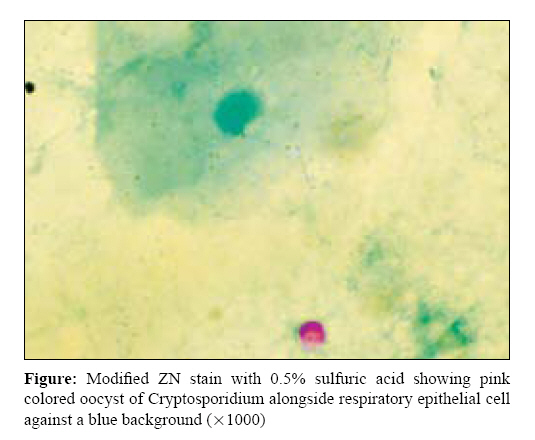
Indian Journal of Medical Microbiology, Vol. 27, No. 2, April-June, 2009, pp. 172-174 Correspondence Cryptosporidial oocysts in gastric aspirate of an infant Rani H, Gupta V, Gulati N, Chander J Department of Microbiology, Government Medical College and Hospital, Sector 32, Chandigarh 160 030 Date of Submission: 25-Aug-2008 Code Number: mb09055 PMID: 19384051 DOI: 10.4103/0255-0857.49441 Dear Editor, Cryptosporidium is an intestinal coccidian protozoan parasite and is a well-known cause of enteritis in acquired immunodeficiency syndrome (AIDS) patients and in children. The most commonly encountered species in human beings is Cryptosporidium parvum. Cryptosporidiosis is associated with significant morbidity and mortality, especially among individuals who are immunosuppressed and infants and children in the developing world. There are reports of intestinal cryptosporidiosis in both malnourished as well as nourished children of < 2.5 years of age. [1] There are reports in the literature indicating that respiratory symptoms occur with a considerable frequency in subjects with intestinal cryptosporidiosis, although the aetiology of the respiratory symptoms was never investigated. [2] This under-reporting may be because of lack of systematic investigations. The mainstay of diagnosis is modified acid fast staining of stool or other samples for the presence of oocysts of Cryptosporidium. In this report, we describe a new case of cryptosporidiosis in which oocysts of Cryptosporidium were detected from an unusual specimen, i.e., gastric aspirate. An 8-month-old male child presented to the paediatric emergency ward, Government Medical College and Hospital, Chandigarh (north India) on 2 November 2007 with complaints of fever and pain in the abdomen since 5-6 days, cough and coryza since 3 days and fast breathing since 1 day. He had abdominal distension and passage of loose stools since 1 month of age and was also not gaining weight. The child was from a poor socioeconomic background. His immunization and dietary history were non-contributory. He was the first issue of his parents and was delivered normally with no complication. On examination, the abdomen was found to be soft and non-tender but distended. There was no palpable organomegaly. The respiratory rate was 60/min. Bilateral air entry was present with ronchi and crepts. The cardiovascular and central nervous systems were within normal limits. The total leucocyte count was slightly raised with mild neutrophilia. In peripheral blood smear, the red blood cells showed mild anisocytosis, poikilocytosis and hypochromasia. The neutrophils showed toxic granulations and platelets were adequate in number. The liver function test was normal. X-ray of the abdomen showed dilated small bowel loops and no air-fluid levels were noticed. An ultrasonogram of the abdomen also showed dilated bowel loops in the left lumbar region. X-ray of the chest showed hyperinflation of the lungs with some hazy opacity. The child was diagnosed as a case of malabsorption syndrome with pneumonitis. The child was nebulized and started with antibiotics (cefotaxime, gentamicin, cloxacillin) for pneumonitis. Initially, respiratory distress persisted with both inspiratory and expiratory ronchi but after 3-4 days, respiratory distress improved slightly. Thus, the patient was continued with the same treatment. Abdominal distension persisted. A nasogastric tube was put to decompress the abdomen. The child was passing loose, greenish stools five to six a day and also had hypokalaemia and hypocalcaemia. The patient was investigated for malabsorption syndrome. Microscopic examination of the stool showed no trophozoite, cyst, ova, larva or adult parasite. Neutrophils were slightly raised (7-8/hpf) in the stool sample. Tissue transglutaminase IgA was also estimated to rule out coeliac disease, and it was negative. Blood and urine culture of the child were also sterile. The human immunodeficiency virus status of the mother was tested and was found to be non-reactive. Further investigations to ascertain the immunological status could not be carried out because of financial constraints. The child was investigated for pulmonary tuberculosis in view of persisting respiratory distress. The gastric aspirate was sent to the microbiology department for staining for acid fast bacteria (AFB). Antituberculosis treatment was then started empirically on the seventh day of admission considering persisting respiratory distress. On examination of the acid fast-stained smear of the gastric aspirate, some faint pink-coloured rounded structures were seen. Keeping the possibility of Cryptosporidium, in mind modified Zeihl-Neelsen staining using 0.5% sulphuric acid was performed. It revealed oocysts of Cryptosporidium, as shown in the [Figure - 1]. After confirming our findings, the stool sample of the patient was also examined for oocysts and it was also found to be positive. The treating paediatrician was informed about the diagnosis. Further management of the child could not be performed as the parents left against medical advice. There are few case reports of respiratory cryptosporidiosis in immunocompetent children, but the PubMed search did not reveal any case report in which Cryptosporidium was detected from gastric aspirate. The samples that have been tested for the diagnosis of respiratory cryptosporidiosis are induced sputum, bronchoalveolar lavage and tracheal or bronchial tissue. [3] In none of the reports was gastric aspirate tested for Cryptosporidium oocysts. Ours was also an incidental finding while looking for AFB in the gastric aspirate of the infant. Young children, pregnant women and people with a severely weakened immune system are at a risk to develop serious disease. Our finding suggests that the index child could either be suffering from intestinal cryptosporidiosis only and finding of oocysts in the gastric aspirate could be due to reverse peristalsis or, because the child had respiratory symptoms and infiltrates in the lung on X-ray chest examination, he could be having pulmonary involvement with Cryptosporidium. Thus, gastric aspirate can be one of the useful specimens for looking for Cryptosporidium, especially in children. Collection of gastric aspirate is much easier and more economical than doing bronchoscopy for bronchoalveolar lavage and tissue specimen. It can be routinely practiced, especially in children of intestinal cryptosporidiosis presenting with respiratory symptoms. This can also improve the under-reporting of cases of respiratory cryptosporidiosis. The literature also points out to the transient respiratory infection of the respiratory tract in immunocompetent children with intestinal disease.[2] The second important finding pertaining to our case is the demonstration of Cryptosporidium from an otherwise immunocompetent infant. Thus, our finding highlights the importance of gastric aspirate as an important specimen for diagnosing pulmonary involvement in intestinal cryptosporidiosis and also the possibility of both intestinal and extraintestinal cryptosporidiosis even in an immunocompetent host. Acknowledgement We thank the Department of Parasitology, PGIMER, Chandigarh, for confirming our finding.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09055f1.jpg] |
| |||||||||
{kind=link}