 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
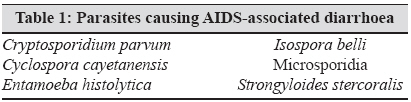
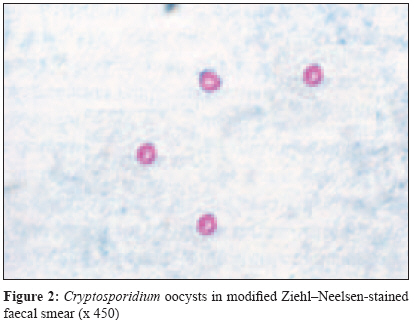
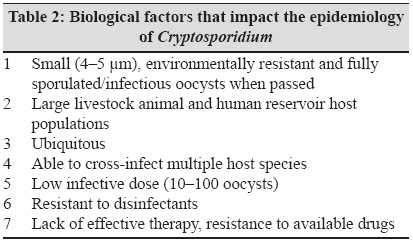
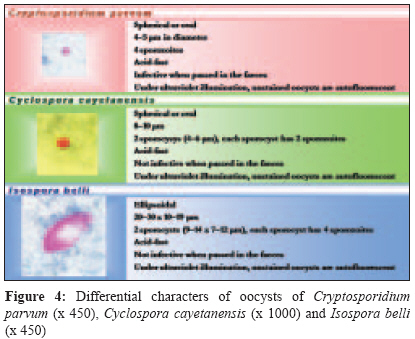
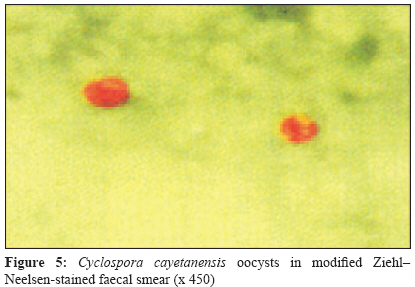
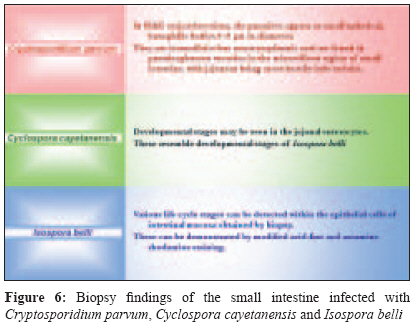
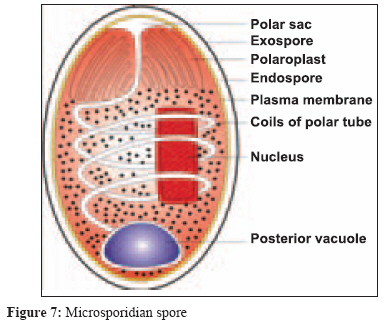
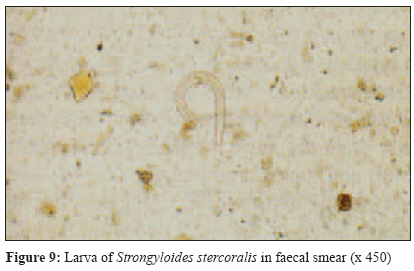
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 185-190 Review Article AIDS - associated parasitic diarrhoea Arora DR, Arora B Department of Microbiology, Medical College, Agroha, Hisar - 125 047 Date of Submission: 23-Jun-2008 Code Number: mb09060 PMID: 19584497 Abstract Since the advent of human immunodeficiency virus infection, with its profound and progressive effect on the cellular immune system, a group of human opportunistic pathogens has come into prominence. Opportunistic parasitic infection can cause severe morbidity and mortality. Because many of these infections are treatable, an early and accurate diagnosis is important. This can be accomplished by a variety of methods such as direct demonstration of parasites and by serological tests to detect antigen and/or specific antibodies. However, antibody response may be poor in these patients and therefore immunodiagnostic tests have to be interpreted with caution. Cryptosporidium parvum , Isospora belli , Cyclospora cayetanensis , Microsporidia, Entamoeba histolytica and Strongyloides stercoralis are the commonly detected parasites. Detection of these parasites will help in proper management of these patients because drugs are available for most of these parasitic infections.Keywords: Cryptosporidium parvum, Cyclospora cayetanensis, diarrhoea, Entamoeba histolytica, HIV/AIDS, Isospora belli, Microsporidia, Strongyloides stercoralis Patients with human immunodeficiency virus (HIV) disease, during the course of their illness, become a MICROBIAL ZOO. Most of the patients with HIV disease die of infections other than HIV. Because of a progressive decline in their immunological responses, patients with HIV infection are extremely susceptible to a variety of common as well as opportunistic infections. [1] Opportunistic parasitic infections can cause severe morbidity and mortality. Because many of these infections are treatable, an early and accurate diagnosis is important. This can be accomplished by a variety of methods such as direct demonstration of the parasite and by the serological tests to detect antigen and/or specific antibodies. Antibody response may be poor in acquired immunodeficiency syndrome (AIDS) patients and, therefore, immunodiagnostic tests have to be interpreted with caution. [2] Parasites causing AIDS-associated diarrhoea are presented in [Table - 1]. Detection of these parasites will help in proper management of these patients because drugs are available for the treatment of most of these opportunistic infections. [1],[2],[3],[4],[5],[6] Cryptosporidium parvum The first reported description of C. parvum was in 1907 in the gastric crypts of a laboratory mouse (Tyzzer). Subsequently, it has been found in chickens, turkeys, mice, rats, guinea pigs, horses, pigs, calves, sheep, rhesus monkeys, dogs, cats and humans. Cryptosporidiosis is a zoonosis and is transmitted by the faecal-oral route. This infection is now well recognized as causing disease in humans, particularly those who are in some way immunosuppressed or immunodeficient. Cryptosporidiosis has been implicated as one of the more important opportunistic infections in patients with AIDS. Calves and perhaps other animals serve as potential sources of human infections . [7] C. parvum undergoes both asexual (schizogony) and sexual (gametogony) multiplication [Figure - 1] in a single host (man, cattle, cat or dog). Man acquires infection by ingestion of food and drinks contaminated with faeces containing oocysts of the parasite. The sporozoites are released in the small intestine, invade the mucosal cells and undergo asexual and sexual multiplication. The end product of the sexual multiplication is the formation of the oocysts. These are released in the lumen of the intestine and excreted in the faeces. These are infective when passed in faeces and the cycle is repeated. Intracellular stages of C. parvum reside within parasitophorous vacuoles in the microvillous region of the host cell. On the other hand, Isospora spp. occupy the parasitophorous vacuole deep (perinuclear) within the host cell. [1] C. parvum in an immunocompetent host causes a self-limiting infection, with diarrhoea and abdominal pain lasting 1-2 weeks. However, in AIDS patients, it causes profuse and watery diarrhoea. It may produce fluid loss of over 10 L/day. In a study, human colon adenocarcinoma cells (Caco-2 cell monolayers) were used to detect the enterotoxic effect of faecal specimens obtained from 11 patients with enteric cryptosporidiosis. Enterotoxic activity was observed in most patients with enteric cryptosporidiosis and was strictly associated with secretory diarrhoea. [8] Cryptosporidiosis is not always confined to the gastrointestinal tract. Additional symptoms (respiratory cryptosporidiosis, cholecystitis, hepatitis and pancreatitis) have been associated with extraintestinal infections. [1] For diagnosis, three consecutive specimens of stool should be examined. A direct wet mount of stool shows highly refractile, spherical or oval oocysts measuring 4-5 mm in diameter. These can be stained by a modified acid-fast staining [Figure - 2], auramine-rhodamine, acridine orange and immunofluorescent antibody. Cryptosporidial antigen in the faecal sample can be detected by the enzyme-linked immunosorbent assay (ELISA). Polymerase chain reaction (PCR) is more sensitive and easier to interpret but requires more "hands-on" time and expertise and is more expensive. Various life cycle stages of the parasite can be detected in the microvillous region of the intestinal mucosa obtained by biopsy, with jejunum being the heavily infected site. [1] Biological factors that impact the epidemiology of Cryptosporidium are given in [Table - 2]. Because no effective therapy for cryptosporidiosis has been identified, therefore, detection of this parasite in immunocompromised hosts, especially those with AIDS, usually carries a poor prognosis. [7] The reduction or elimination of oocysts from the environment forms the mainstay of control of cryptosporidiosis, but is difficult. Freezing and heating at 65 o C for 30 min kills the oocysts. The care to avoid contamination of food and water with faecal oocysts prevents transmission of infection to man. Hand washing, use of gloves and improved personal hygiene minimise the risk of acquiring the infection in the hospital. Isospora belli I. belli was first discovered by Virchow in 1860 and was named by Wenyon in 1923. It is the sporozoan of the human intestine. It is endemic in Africa, Asia and South America. The frequency of I. belli infection in Haitian AIDS patients is 15%, whereas data from Los Angeles during 1985-1992 suggests isosporiasis in 0.78% of the AIDS patients. [8] Man acquires infection by ingestion of food and drinks contaminated with the oocysts of I. belli . The life cycle of this parasite is shown in [Figure - 3]. Infection with I. belli may be asymptomatic or it may lead to a mild self-limiting diarrhoea lasting for 6 weeks to 6 months. Persistent nonbloody diarrhoea indistinguishable from that caused by microsporidia and C. parvum is the major manifestation in AIDS patients. Vomiting, headache, fever and malaise may also be present and dehydration follows when diarrhoea is severe. In AIDS cases, extraintestinal infections can occur, although they are rare. Necropsy occasionally reveals infection of mesenteric lymph nodes, liver and spleen. Biliary disease has also been reported. [1] Laboratory diagnosis of isosporiasis can be carried out by the demonstration of I. belli oocysts in the faeces by examination of unstained or iodine-stained direct smear preparations and by zinc sulphate as well as formalin-ether concentration methods. Oocysts can also be detected in faecal smears after acid fast staining or staining with auramine-rhodamine. Oocysts tentatively detected using auramine-rhodamine stains should be confirmed by wet mount smear examination or acid fast stain, particularly if the stool contains other cells or excess artifact material. With acid fast stain, oocysts appear red in colour. Unstained oocysts are autofluorescent, appearing violet under ultraviolet light and green under green or blue-violet light [Figure - 4]. [7] Various life cycle stages of the parasite can be detected within the epithelial cells of the intestinal mucosa by biopsy. These can be demonstrated by modified acid fast and auramine-rhodamine staining. It is quite possible to have a positive biopsy but not recover the oocyst in the stool because of the small number of organisms present. A highly sensitive and specific method for diagnosis has employed PCR with primers for the small-subunit rRNA sequence of I. belli . [1] Because transmission is via the infective oocysts, prevention centres on improved personal hygiene and sanitary conditions to eliminate possible faecal-oral transmission from contaminated food, water and possibly environmental surfaces. Cyclospora cayetanensis In recent years, human cyclosporiasis has emerged as an important infection, with a number of outbreaks being reported in the United States and Canada. The distribution is worldwide (United States, Caribbean, Central and South America, Southeast Asia, eastern Europe, Australia and Nepal). Cyclospora cayetanensis has been found in the faeces of immunocompetent travellers to developing countries, immunocompetent subjects with no travel history and patients with AIDS. [8] Man acquires infection by ingestion of food and drinks contaminated with faeces containing oocysts of Cyclospora cayetanensis. The life cycle, although not completely understood, is thought to be similar to that of I. belli . In a normal host, it causes a self-limiting infection, with diarrhoea (3-4 days) and abdominal pain . In an AIDS patient, the diarrhoea may persist for 12 weeks or more. Biliary disease has also been reported. Laboratory diagnosis can be carried out by examination of wet smear, modified acid fast staining [Figure - 4] and [Figure - 5] and staining with saffranine. The oocysts of C. parvum and Cyclospora cayetanensis are spherical or oval, measuring 4-5 mm and 8-10 mm respectively, while those of I. belli are large (20-33 mm x 10-19 mm), and are ellipsoidal [Figure - 4]. [1],[2],[3],[4],[7],[9] In the biopsy specimen, developmental stages may be seen in the jejunal enterocytes. These resemble the developmental stages of I. belli. [1] I. belli , Cyclospora cayetanensis and C. parvum are transmitted by the Faecal-oral route with infective oocysts being ingested. The oocysts of I. belli and Cyclospora cayetanensis are not infective when passed in the faeces. They require 3-4 and 5-13 days respectively in the environment to mature. The oocysts of C. parvum , on the other hand, are infective when excreted in the faeces. Differential characters of the oocysts and the biopsy findings of the small intestine in infection with C. parvum, Cyclospora cayetanensis and I. belli are given in [Figure - 4] and [Figure - 6] respectively. [1] Because this parasite, like Cryptosporidium , is not killed by routine chlorination, drinking water treated by halogenations may not be safe. Boiling is recommended. Fresh fruits and vegetables should be thoroughly washed and/or peeled before eating. [7] Microsporidia Microsporidia are unicellular obligate intracellular protozoan parasites. In host cells, the parasites develop and multiply producing a large number of spores. Spores are highly resistant, the only life cycle stage able to survive outside the host cell and is the infective stage. They are small, ranging from 1.5 to 2.5 mm x 2.5 to 4 mm. They are oval to cylindrical and possess a thick double-layered spore wall [Figure - 7] that renders it environmentally resistant. The outer layer, or exospore, is proteinaceous and electron-dense and the inner layer, or endospore, is chitinous and electron-lucent. The plasma membrane lines the inside of the spore wall. Within the cytoplasm the spore possesses a coiled polar tube. It has a spring-like tubular extrusion mechanism by which the infective material "sporoplasm" is injected into the host cell. The microsporidia multiply extensively within the host cell cytoplasm. [9] The life cycle includes repeated divisions by binary fission (merogony) or multiple fission (schizogony) and spore production (sporogony). Both merogony and sporogony can occur in the same cell at the same time. During sporogony, a thick spore wall is formed, providing environmental protection for this infectious stage of the parasite. [7] Microsporidia have been recognized as causing disease in animals as early as 1920s, but were not recognized as agents of human disease until the AIDS pandemic began in the mid 1980s. Currently, 15 microsporidian species have been identified in man, of which most, but not all, are associated with HIV infection. Infection is probably by spores being ingested, inhaled or inoculated (eyes). The spores are highly resistant in the environment. Transplacental transmission also occurs. [7] Intestinal microsporidiosis is the most common infection caused mainly by Enterocytozoon bieneusi . It produces persistent diarrhoea with wasting. It is normally restricted to the small intestinal enterocytes whereas E. intestinalis spreads into the lamina propria. Both these species have been found to spread from the intestine along the epithelium to the gall bladder and the pancreatic and bile ducts. Although rarer, spread to the respiratory system has been documented with both species. In AIDS patients, ocular involvement is often the presenting sign of microsporidiosis. [1] Enteric infections can be diagnosed by light microscopic and electron microscopic examination of the small intestinal biopsy sections or touch preparations of biopsies. Tiny intracytoplasmic spores are best demonstrated by Brown-Brenn Gram stain, Giemsa or PAS staining. They stain poorly with H and E stain. Electron microscopy (EM) is the "gold standard" for confirming infection and attempting to classify the organisms seen in tissues. However, this option is not available to all laboratories and sensitivity of EM may not be equal to that of other methods when examining stool or urine. [7] Microsporidial spores in the stool samples and the contents of the duodenum-jejunum using the Entero-Test method can be detected by staining with modified trichrome stain, Giemsa or fluorescent dyes. These can also be detected by indirect immunofluorescence antibody stains using polyclonal antisera. Microsporidial spores can also be detected in urine and nasopharyngeal swabs by the above staining techniques. [1] Microsporidial spores from clinical specimens such as urine, nasal polyps, nasopharyngeal aspirates, faeces and muscle biopsies can be cultured in various cell lines. Microsporidial DNA can be amplified by PCR [1] A variety of serologic tests [carbon immunoassay, indirect immunofluorescent-antibody (IFA) test, ELISA, counterimmunoelectrophoresis and Western blotting] have been used to detect immunoglobulin (Ig) G and IgM antibodies to Microsporidia, particularly to E. cuniculi . IFA and ELISA have been the most useful because of the simplicity of the test methods. [7] The presence of infective spores in human clinical specimens suggests that precautions when handling body fluids and personal hygiene measures such as hand washing may be important in preventing primary infections in health care settings. Strongyloides stercoralis S. stercoralis was first identified by Normand in 1876 in the faeces of French troops who had been suffering from uncontrollable diarrhoea in Indochina. [10] It is worldwide in distribution. However, it is more common in the tropics and subtropics, including those of Africa, South America and Asia, including India. It has been estimated that there are 80-100 million cases of strongyloidiasis worldwide. It is an important opportunistic pathogen in an immunocompromised host. [7] Prevalence of S. stercoralis infection in India varies from 0.68% [11] to 3.0%. [12] The most common mode of transmission of Strongylodes in India (in both man and animals) is through the consumption of contaminated water and soil. [11] Adult female S. stercoralis lives buried under the mucosa of the small intestine, especially in the duodenum and the jejunum. The life cycle of S. stercoralis is given in [Figure - 8]. In a normal host, S. stercoralis causes asymptomatic to mild abdominal symptoms. It can remain latent for many years owing to the low-level infection maintained by the internal autoinfective life cycle. In an AIDS patient, it can result in disseminated disease (hyperinfection syndrome due to the autoinfective nature of the life cycle). During hyperinfection, filariform larvae may enter arterial circulation and lodge in various organs, e.g. lymph nodes, endocardium, pancreas, liver, kidneys and brain. It may cause abdominal pain, pneumonitis, episodes of unexplained bacteraemia or meningitis with enteric bacteria and unexplained eosinophilia, which may range from 10% to 15%. [1],[13],[14],[15],[16] Very rarely, in an immunosuppressed host, colonization may mimic gastrointestinal tumour mass. [17],[18] Laboratory diagnosis of S. stercoralis infection can be carried out by the demonstration of rhabditiform larvae, filariform larvae [Figure - 9] and parasitic adult females of S. stercoralis in Papanicolaou-stained smears of faeces, duodenal aspirates or sputum. If signs of meningitis are present, the cerebrospinal fluid must invariably be examined for larvae and pyogenic bacteria. [14],[15],[16] Sometimes, unhatched eggs are found, which cause confusion with hookworm eggs. [10] Use of the Baermann technique and agar plate culture may increase the diagnostic yields of faecal examination. [1],[19] During hyperinfection with dissemination, Strongylodes larvae can be detected in a variety of body fluids and tissues. [1] Eosinophilia may be present, but its absence does not exclude the diagnosis. Serological diagnosis of S. stercoralis infection can be carried out by ELISA, indirect haemagglutination and indirect immunofluorescence. Intestinal biopsy may reveal adult females, well-segmented eggs and numerous larvae. The bowel lining becomes congested and oedematous, with possible ulcerations. Chronic infection may reveal bowel wall fibrosis. [1] For prevention of strongyloidiasis, contact with contaminated infective soil, faeces or surface water should be avoided. Sanitary disposal of faeces to prevent contamination of soil, personal hygiene measures such as hand washing and safe drinking water supply are very important. Because all infected individuals are at risk for hyperinfection and disseminated disease, the identification of people who may have contracted their infection many years earlier is of great clinical significance. Individuals found to have infection should be treated. [7],[10] References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09060f6.jpg] [mb09060f9.jpg] [mb09060t1.jpg] [mb09060f4.jpg] [mb09060f1.jpg] [mb09060f3.jpg] [mb09060f8.jpg] [mb09060f7.jpg] [mb09060f2.jpg] [mb09060f5.jpg] [mb09060t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}