 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
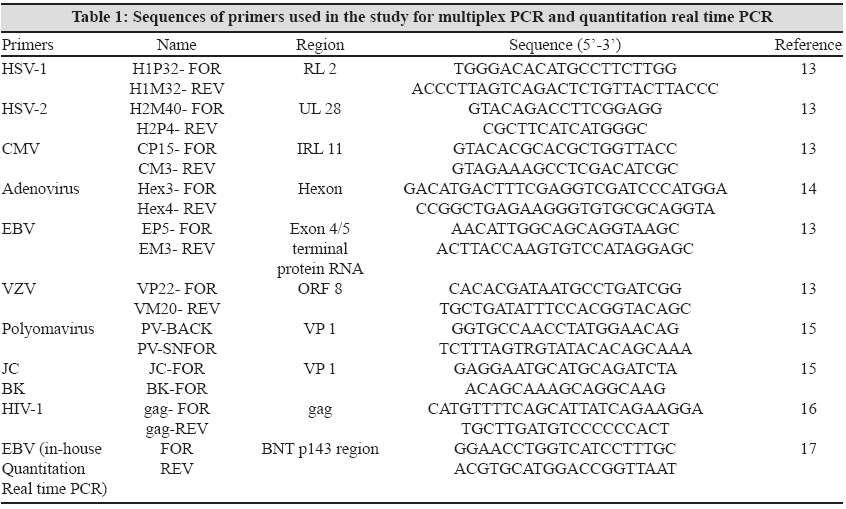
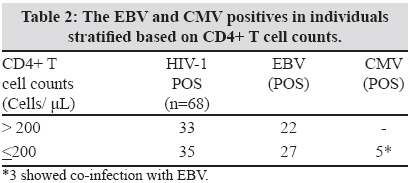
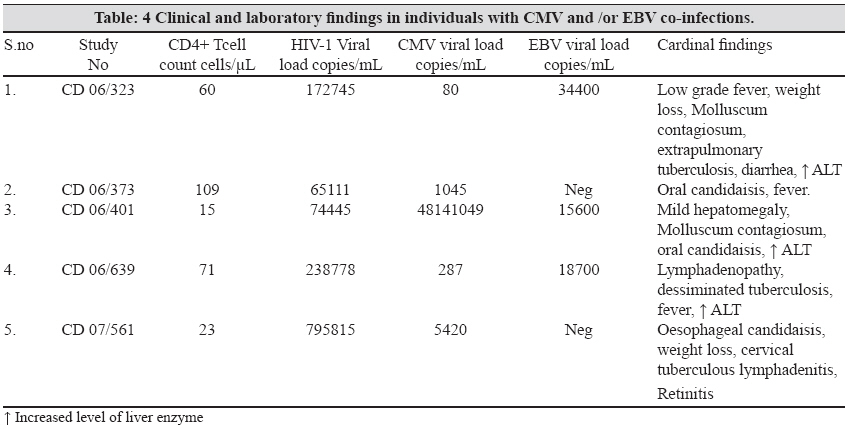
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 210-216 Original Article Detection of opportunistic DNA viral infections by multiplex PCR among HIV infected individuals receiving care at a tertiary care hospital in South India Sachithanandham J, Ramamurthy M, Kannangai R, Daniel HD, Abraham OC, Rupali P, Pulimood SA, Abraham AM, Sridharan G Department of Clinical Virology, Christian Medical College, Vellore - 632004 Date of Submission: 28-Dec-2008 Code Number: mb09063 PMID: 19584500 Abstract Purpose: Opportunistic viral infections cause increased morbidity and mortality among human immunodeficiency virus (HIV) infected individuals, especially those who are not on antiretroviral treatment. Early diagnosis of these opportunistic viruses will be able to reduce the risk of disease progression with appropriate intervention.Materials and Methods: Multiplex PCR was attempted to detect the opportunistic herpes viruses (HSV-1, HSV-2, VZV, EBV, and CMV), adenovirus and polyoma viruses (JC and BK) in three cocktails of PCR reactions. Subsequently, all the viruses detected were quantitated by testing using monoplex real time PCR. Whole blood samples collected between 2006 and 2007 from 68 treatment naοve HIV-1 infected and 30 normal healthy individuals were tested for these eight viruses. Among the 68 HIV -1 infected individuals 35 had CD4+ T cell count less than or equal to 200 while the other 33 had greater than 200 CD4+ T cells. Results: Among the 68 HIV-1 infected individuals, 49 (72%) were positive for EBV, 5 (7%) samples were positive for CMV. All the five CMV positive individuals had CD4+ T cell count of less than or equal to 200 cells/µL. The mean EBV load among the individuals with a CD4+ T cells of less than or equal to 200 cells/µL was 3.88 log 10 while among those with greater than 200 CD4+ T cells it was 3.75 log 10 . The mean CMV load was 6.98 log 10. Three samples were positive for both CMV & EBV. None of the samples was positive for HSV-1, HSV-2, VZV, Adenovirus, JC and BK viruses. Conclusions: In our study, multiplex PCR based detection system was found useful in detecting opportunistic viruses in HIV infected individuals. Though EBV is the most prevalent opportunistic viral infection among HIV infected individuals, there was no significant association between EBV load, CD4+ T cell counts and HIV-1 virus load. CMV was seen in HIV infected individuals with low CD4+ T cell counts (less than 200 cells/μL). Keywords: Human immunodeficiency virus, India, multiplex polymerase chain reaction, opportunistic viruses Introduction In HIV infected individuals, opportunistic viral infections are the major cause of morbidity and mortality. These agents cause infections which could be asymptomatic or mildly symptomatic in immunocompetent individuals, and it is often self- limiting. However, in immunosuppressed individuals and individuals with malignancy, infection with these agents leads to severe life-threatening diseases. [1],[2] The primary target of HIV during infection is CD4+ cells that lead to reduction in CD4+ T cells and thereby cause immunosuppresion. During HIV disease progression infection, there will be reduction of CD4+T cells and the infected individuals could succumb to AIDS related opportunistic viral infections when CD4 cells are less than 200cells/µL. [3] The important opportunistic viruses that can cause infection in HIV infected individuals are herpes viruses like HSV, VZV, EBV and CMV. Herpes virus infections are seen in HIV infected individuals and can manifest as meningitis, encephalitis, oral hairycell leukoplakia (OHL), lymphoproliferative disorders, retinitis. [4],[5] One another important herpes virus that can cause Kaposi′s sarcoma associated lesions in HIV infected individuals is the human herpes virus-8 (HHV-8). [6] Polyomaviruses like the JC virus causes progressive multifocal leucoencephalopathy in HIV infected individuals. [7] Infections associated with adenovirus in HIV infected individuals manifest as lethal pneumonia, diarrhoea and encephalitis. [8] In HIV infected individuals, the detection of these opportunistic viruses and specific treatment are very important to effectively prevent their deleterious effects. There were several techniques to detect these opportunistic viruses, such as cell culture for isolation, Enzyme Linked Immunosorbent Assay (ELISA) for antigen or antibody detection, and Polymerase Chain Reaction (PCR) for nucleic acid detection. [9],[10] Cell culture isolation has limited scope because some viruses cannot easily be grown in culture (JC and BK) and is also time consuming. ELISA, though not expensive, has some drawbacks like pre-exposure to viruses like CMV; EBV reduces the specificity for the episode of illness. The PCR is very useful in screening for these opportunistic viruses and a multiplex assay has an additional advantage of screening for these opportunistic viruses since it involves the simultaneous amplification of one or more targets. It also enables a wide range of samples to be tested, like blood, CSF, urine. [10] Many recent studies have shown the importance of using whole blood rather than fractions for testing for viral infections, especially in the case of CMV. [11] Early detection is very important in treating opportunistic infections and there are many drugs to improve the survival of such patients. [12] Materials and Methods This study was carried out at the department of Clinical Virology of a tertiary care teaching hospital in South India between 2006 and 2007. Whole blood samples were collected from individuals with HIV-1 established infection who are not receiving antiretroviral therapy (ART). Sixty eight HIV-1 infected individuals who reported to the virology department for the CD4+ T cell estimation and or viral load tests were included in this study. We also collected whole blood samples from 30 normal healthy controls. At the time of sample draw, the HIV-1 infected individuals were not specifically diagnosed to be ill with any opportunistic viral infection by the referring clinician. All the study volunteers were enrolled in the study after a written informed consent for HIV related testing by a UNAIDS approved HIV antibody test. Sample collection Multiplex PCR Cell culture supernatants were used as the sources of positive controls for viruses like CMV, HSV-1, HSV-2, EBV and adenoviruses. Live attenuated vaccines (Oka strain) were used to extract VZV DNA, while plasmids were used for JC and BK (John Hopkins University, Baltimore, USA). Sterile doubled distilled water was used in PCR testing after every third sample as negative control to check for cross contamination. For the detection of these eight viruses, their multiplex PCR reactions protocol were as follows: Cocktail-1 (CMV, HSV-2 and HSV-1) was performed using 2.5 units of hot start Taq polymerase (Qiagen), 0.2mM dNTPs and 20 picomoles of primers each in a reaction volume of 50μl. Cocktail-2 (VZV, EBV and Adenovirus) was performed using 2.5 units of hot start Taq polymerase (Qiagen), 0.4mM dNTPs and 20 picomoles of primers each in a reaction volume of 50μl. Cocktail-3 (JC and BK) was performed using 3.5 units of hot start Taq polymerase (Qiagen), 0.4 mM dNTPs and 25 picomoles of primers each in a reaction volume of 50μL. Five microliters of extracted DNA was added to the total reaction volume of 50μL for each cocktail. The multiplex PCR thermal cycling condition for all three cocktails was performed with the initial Taq activation temperature of 95°C for 15 minutes. Subsequently, Cocktail -1 was cycled at 94°C for 30 sec, 52°C for 40 sec, 72°C for 50 sec for 40 cycles and final extension at 78°C for 15 min. Cocktail -2 was cycled at 94°C for 45 sec, 57.5°C for 50 sec, 72°C for 70 sec for 40 cycles and final extension at 72°C for 7 min. Cocktail -3 was a hemi nested PCR with two rounds of amplification. In the first round, amplification cycling conditions were 94°C for 3 min, 94°C for 20 sec, 53°C for 20 sec and 72°C for five min for 30 cycles. The cycling conditions of second round heminested PCR was also the same except for a change in the annealing temperature of 58°C for 20 sec. All the assays for the three cocktails were amplified using thermal cycler Gene amp PCR system 2400 (Perkin Elmer, Massachusets, USA) or PTC-100 (MJ Research, California, USA). The amplified products were detected by 2% agarose gel in 1X TBE containing 0.5µg/ml ethidium bromide (Sigma, St. Louis, USA) in agarose gel electrophoresis unit. The gels were viewed in a UV Transilluminator (Mighty Bright, Hoefer Scientific Instruments, San Francisco, USA) and photographed using Gel documentation 2000 (Bio Rad, California, USA). The expected specific product sizes for all target genes (amplicons) of the viruses were as follows: Cocktail-1, HSV-1 -147 bp, HSV-2 -227 bp, and CMV 256 bp; Cocktail-2 VZV -275 bp, EBV -182 bp and adenovirus -139 bp and Cocktail-3 JC -199 bp and BK -246 bp respectively. All the samples negative for all the viruses were also tested for α tublin gene to check the integrity of DNA in the sample. The lower detection limit for the PCR was estimated for all the eight viruses. CD4+ T cell estimation In-house HIV-1 RNA PCR EBV Quantitation PCR CMV Quantitation PCR assays Validation of the PCR assays Statistical analysis Results The 30 normal healthy controls were negative for HIV antibody. Among the 68 samples from HIV-1 infected individuals, 49 (72%) samples were found to be positive for EBV. Nineteen samples were negative by all three cocktails. These 49 samples were repeated again by EBV uniplex PCR to confirm EBV positive status. In 49 EBV positive individuals, 27 had CD4+ T cell counts less than or equal to 200 cells /μL (range 6-186 cells /μL) and 22 had CD4+ T cell counts greater than 200 cells /μL (range of 202-845 cells /μL). Samples of 5 (7%) individuals were positive for CMV. Among these, three samples showed co-infection with EBV. All the CMV positive patients had a CD4+ T cell count of less than or equal to 200 cells /μL. The data on EBV and CMV positivies based on the CD4+ T cell counts are shown in [Table - 2]. Among the 30 healthy controls one individual was positive for EBV. The frequency of EBV and CMV positivies in individuals with CD4+ T cell count less than or equal to 200 and greater than 200 cells/μL was compared. There was no significant difference between the two groups for EBV positivity (p = 0.33). However, for CMV positivity it just fell short of significance (p =0.07). The EBV quantitation PCR results in both HIV-1 infected individuals and control group based on the CD4+ T cell counts are shown in [Table - 3]. All the 49 EBV samples were found to be positive and their EBV DNA load ranged from 300 to 543300 copies/ml. The one control sample were found to have EBV DNA load of 5800 copies/ml. There was no significant difference in the viral load level between the two groups of patients stratified by CD4+ T cell counts into less than or equal to 200 or greater than 200 cells/μL. A higher percentage of individuals (77%) who had EBV were found to be having a higher HIV-1 viral load (> 100000 copies/ml). This difference was also not significant (p = 0.26). The mean EBV viral load was 3.68 log10 and 3.91log 10 among individuals with HIV-1 viral load of less than 100000 RNA copies/ml group and > 100000 copies/ml respectively. This difference was not statistically significant (p= greater than 0.05). The CMV DNA load among the five positive individuals ranged between 80-48141049 copies/ml. In five of the 68 individuals HIV-1, RNA was undetectable. Two among these five individuals had a CD4+ T cell count of greater than 200 cells while the other three had less than or equal to 200 cells. The clinical and laboratory findings of the five CMV positive individuals in the study are given in [Table - 4].Discussion Opportunistic viral infections play a vital role in the progression of the disease in HIV infected individuals. The co-infections with these viruses would require specific treatment when immunosuppression advances. Hence, it is important to detect these opportunistic viruses in HIV infected individuals to reduce morbidity and mortality. Since all HIV infected individuals have to be screened for these viruses, it will be economical to use a multiplex PCR. Our data showed that majority (72%) of the HIV infected individuals were positive for EBV. The percentage positives was found to be higher among individuals with CD4 + T cells less than or equal to 200 cells/μL. However, the difference was not significant. In a similar way a higher number of individuals who had EBV showed a HIV-1 viral load of greater than 100,000 copes/μL (77% compared to 65%). Subsequent quantitation of the EBV DNA in all the samples failed to find any significant association between EBV load, CD4+ T cells and HIV-1 viral load level. The patients in our study group failed to show evidence of infection with HSV-1, HSV-2, VZV, adenovirus, JC and BK. One study looked at the prevalence of opportunistic DNA viruses in saliva of HIV infected individuals and found samples positive for HSV-1, CMV, EBV and HHV-8 [18] . The EBV and HHV-8 were found more frequently even in presence of ART. [18] They also showed that EBV and CMV were found to be detected significantly more when the CD4+ T cell counts were less than or equal to 200 cells/μL. Another study had reported that EBV and CMV were commonly detected in CSF samples of HIV infected individuals and some co-infection of CMV with EBV was documented. [19] In our study group among the five CMV positive individuals, one individual had retinitis while another three had increased ALT level suggesting CMV induced hepatitis. It is important to start pre-emptive anti-CMV therapy in patients who are CMV DNA positive to prevent major CMV associated complications like retinitis. However, one of the arguments in this case is that the CMV is detected in blood and hence it may indicate only a latent infection. It will be ideal to standardize a real time PCR to detect immediate early mRNA (IE mRNA) to find active CMV infection. The detection of IE mRNA for CMV is found to be a useful parameter for initiation of preemptive therapy in transplant recipients. [20] Also, this is a laboratory based cross sectional study and hence the in-use utility of the assays could be established only in long term cohort of HIV infected individuals to assess the likelihood ratios of the assays. Stevens et al . (2001) have reported un-fractionated whole blood for EBV detection as the preferred clinical sample in HIV infected individuals, patients with infectious mononucleosis, Burkitt′s lymphoma and lung transplant patients. [11] It is also shown that compared to plasma sample the amount of EBV DNA in whole blood is higher. [21] The level of EBV DNA in whole blood sample of EBV related symptomatic transplant patients are significantly higher than asymptomatic transplant individuals. [21] However this difference was not observed when plasma was used as sample. [21] In our study, we also found high EBV positives when whole blood was tested. The CMV positives in our study were 7.4% and all these individuals had a CD4+ T cell count of less than or equal to 200 cells/μL. These findings are important in light of the earlier report that the presence of CMV and EBV significantly delay the response to ART in HIV-1 infected individuals. [22] This study uses the benefits of multiplex PCR which can amplify many targets in a single reaction tube and with variety of clinical samples. The multiplex PCR has many advantages like saving time, labor, cost effectiveness and ease of performance. One of the drawbacks of our study is the low sensitivity of these assays as the format is essentially a non nested PCR. It is important to increase detection limit of these assays which can be done by doing a nested PCR or a real time PCR with specific probes. [23] However, the multiplexing is comparatively easy with real time PCR. Another advantage of doing real time PCR is the ability to quantify. It is shown for several viruses like CMV, HHV-8 and EBV that there exists an association between copy number of viruses and clinical illness. [21,24] Our study showed significant association between the HIV disease stage by CD4+ T cells and CMV positive status but not EBV. Though there is no association of EBV load and HIV disease stage in our population the effect of EBV positives on response to ART has to be assessed. One study had compared quantitative real time PCR and conventional gel based quantitation PCR assay and obtained very similar results. [25] In their study they also used whole blood samples but from pediatrics transplant individuals. Real time PCR added advantage over conventional PCR by eliminating both post PCR steps and need for diluting samples like EBV, CMV with high viral titers. [25] Development of quantitative real time PCR is very useful for diagnosing the disease and also prediction of the development of disease. This will also help to monitor the antiviral treatment response. Screening of HIV patients for other opportunistic viruses may also help in identifying the patients who may develop IRIS with these. [26] This is the first report from India on viral opportunistic infections detectable in the blood of HIV infected individuals and demonstrates the high association of EBV and CMV with HIV infection. Some viruses like JC, BK were not detected in whole blood. Previous studies have had success with other appropriate samples like CSF and urine respectively. [7] More studies are required to fully understand the implications of these findings. Acknowledgment Bulk of the study was carried out by Intramural (Christian Medical College, Vellore) support. Quantitation PCR carried out for EBV and CMV was supported from a DBT (Government of India) grant received on September 4, 2008.References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09063t4.jpg] [mb09063t2.jpg] [mb09063t1.jpg] [mb09063t3.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}