 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
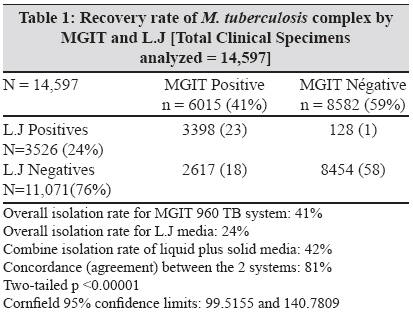
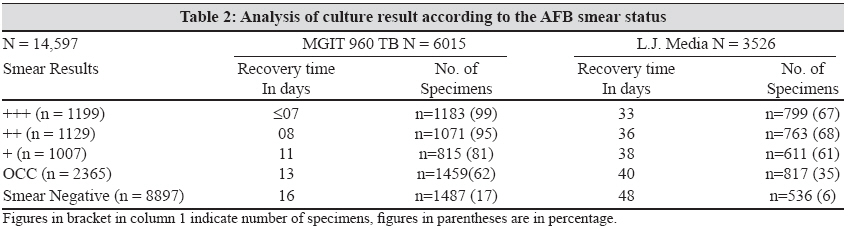
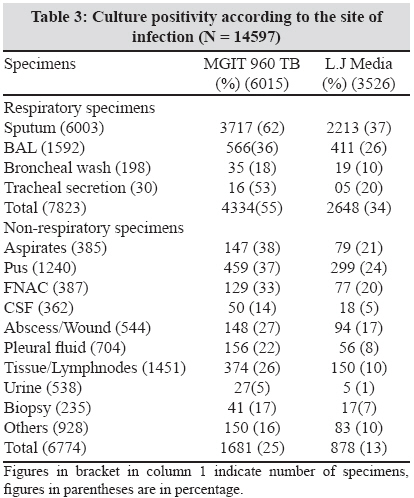
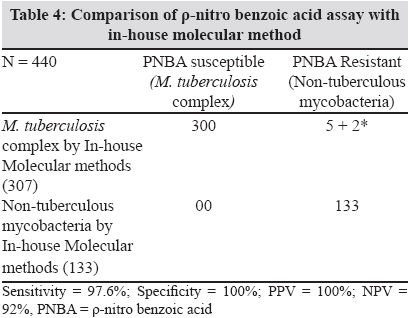
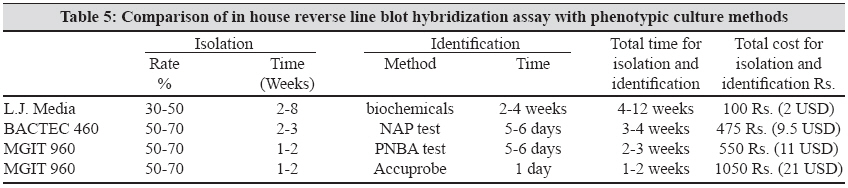
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 217-221 Original Article Evaluation of the bactec MGIT 960 TB system for recovery and identification of Mycobacterium tuberculosis complex in a high volume tertiary care centre Rodrigues C, Shenai S, Sadani M, Sukhadia N, Jani M, Ajbani K, Sodha A, Mehta A Microbiology Section, Department of Lab Medicine, P.D. Hinduja National Hospital & MRC, Mumbai - 400 016 Date of Submission: 30-Dec-2008 Code Number: mb09064 PMID: 19584501 Abstract Aim: To evaluate the performance of an automated BACTEC MGIT 960, a non-radioactive, non-invasive liquid culture system for cultivation of M. tuberculosis complex in terms of recovery rate and time.Materials and Methods: From March 2005 to December 2007, 14,597 specimens were processed using the MGIT 960 system and the results were compared with conventional L.J medium. We standardised r-nitro benzoic acid (PNBA) assay on MGIT 960 TB system for identification of M. tuberculosis complex and evaluated its usefulness by comparing the results with an in-house molecular assay and sequencing. Results and Discussion: Of the total 6143 (42%) isolates positive for M. tuberculosis complex, 6015 (41%) were positive by MGIT 960 TB system. In contrast, 3526 (24%) M. tuberculosis complex isolates grew on the conventional L.J medium. The mean turn around time for mycobacterial growth in smear-positive specimens was nine days for MGIT 960, and 38 days for L.J. medium whereas in smear negative specimens it was 16 days by MGIT vs. 48 days by L.J. Conclusion: MGIT 960 system with PNBA assay for identification of M. tuberculosis complex is a rapid and useful method in laboratories processing a large number of specimens. Keywords: MGIT 960, tuberculosis Introduction Bacteriological confirmation plays a key role in the diagnosis of tuberculosis (TB). The most commonly used conventional Lowenstein Jensen (L.J) culture method requires at least 6-10 weeks of incubation due to the slow growth rate of the Mycobacterium tuberculosis complex. The use of the radiometric BACTEC 460 TB system considerably improves the isolation and decreases the time required to detect mycobacteria. However, this procedure is still labor-intensive and requires attention to special safety and regulatory issues regarding radioisotopes. [1] BACTEC 460 is used in many laboratories worldwide but the increasing cost of radioactive waste disposal promoted the manufacturer to develop alternative systems. . The automated BACTEC Mycobacterial Growth Indicator Tube (MGIT) 960 TB system is a state of the art, in-vitro diagnostic instrument designed and optimized for the rapid detection of mycobacteria from clinical specimens (except blood). This system has a 960-tube capacity for nearly 8000 specimens per year and is useful in laboratories dealing with large specimen loads. [2],[3],[4],[5] It provides continuous monitoring of patient samples to identify the positive ones and refers safe, on-board incubation. MGIT utilizes a modified 7H9 Middlebrook broth base with 0.25% glycerol (7 ml) with an oxygen quenching fluorescent sensor embedded in silicon at the bottom to detect microbial growth directly from clinical specimens. [2] Species identification of all isolated mycobacteria can be done using a r-nitro benzoic acid (PNBA) from MGIT positive vials. PNBA inhibits mycobacteria belonging to the M. tuberculosis complex while other mycobacteria show either slight or no inhibition. The alternative option is commercial molecular techniques, as probe hybridization is very expensive for routine labs in developing countries. In this study, we compared the recovery rate and time of MGIT 960 system versus the conventional L.J media routinely used for AFB culture across India. The efficiency of PNBA assay for identification of M. tuberculosis complex was analysed using 440 culture isolates and results were compared to a r-nitro-a-acetylamino-β -hydroxypropiophenone (NAP) test on BACTEC 460 TB system, an in-house Reverse Line Blot Hybridization (RLBH) assay and sequencing. Materials and Methods All clinical specimens were digested and decontaminated by the standard N -acetyl-L-cysteine-NaOH method. [6] The sediment was suspended in 1 ml of sterile phosphate-buffered saline (pH 6.8). 0.5 ml of the processed specimen was then inoculated into MGIT 960 vials supplemented as described by the manufacturer, and 0.2 ml onto L.J medium slants. All inoculated MGIT vials were incubated in the MGIT 960 instrument either until they were flagged positive by the instrument or for a maximum of six weeks. L.J medium slants were examined daily for the first one week and thereafter, once a week, for twelve weeks, for the visible appearance of colonies. All positive MGIT vials were confirmed for acid fast bacilli by ZNCF staining and further subjected to identification of M. tuberculosis complex, by the PNBA assay. Obvious turbidity in the MGIT vial was confirmed by Gram staining of the smear as well as subculture on blood agar medium. In addition, 0.2 ml of positive broth was subcultured on an additional L.J. slant. Growth on this L.J subculture was used to rule out mixed infection, of MTB and Non Tuberculous Mycobacteria (NTM) strains. Identification using PNBA: It has been reported that the growth of MTB isolates is inhibited by PNB 500 mg/ml whereas NTM are resistant to this concentration. The PNB stock solution was prepared to ensure a final concentration of 500 mg/ml in the MGIT vial. [7],[8],[9] This stock solution was aliquoted and stored at -20 0 . The PNBA test was performed by inoculating the positive culture into two MGIT tubes with and without PNBA and incubated in the MGIT 960 system. The growth Control (GC) was flagged positive by the MGIT system when Growth Unit reached 400. Cut off points of les than or equal to 100 was taken as sensitive indicating the growth of M. tuberculosis complex. Any value more than 100 was considered resistant indicating NTM. All samples showing resistance or error status were further tested by NAP test on BACTEC 460 TB instrument. [10] Further validation of the PNBA results was performed using an in-house reverse line blot hybridization method [11] in 440 cases. In this method, 564 bp region of rpoβ gene was amplified and hybridized with different probes specific for 15 different clinically relevant species. [11],[12] All representative strains of each species and mixed infection as well as all controversial results were confirmed by sequencing. Quality Control (QC): QC of the MGIT medium and PNBA was carried out using STD H 37 RV and ATCC strains of M. tuberculosis complex and NTM ( M. smegmatis and M. intracellulare .) Results A total of 14597 clinical specimens were analysed using MGIT 960 TB system from March 2005 to December 2008 and results were compared with the conventional L.J method. About 7823 (54%) were collected from patients suspected of having pulmonary TB and 6674 (46%) were from patients suspected of having extra-pulmonary TB. M. tuberculosis complex was isolated in 6143 (42%) cases whereas NTM were detected in 203 (1.4%) cases [Table - 1]. By both the culture methods, 3398 (23%) specimens were positive for M. tuberculosis complex. An additional 2617 (18%) cases were positive only by MGIT 960 TB system. Of the 128 (1%) MGIT negative L.J. positive cases, 83 were negative by MGIT whereas in 45 cases either NTM or contaminants like gram positive cocci were isolated by MGIT and M. tuberculosis complex was isolated on L.J. Of the 8454 cases negative for M. tuberculosis complex by both the methods, 8286 were clearly, no growth, whereas 168 were NTM. Comparison of recovery rate and time taken by both the methods as per AFB smear status of clinical specimens was described in [Table - 2]. Of the 1199, highly smear positive (3+) specimens, 99% were positive in less than seven days by MGIT 960 TB system whereas only 67% were positive by L.J in 33 days. The mean turn around time for mycobacterial growth in all smear-positive specimens was nine days for MGIT 960, and 37 days for L.J. medium. In case of smear negative specimens, of the 8897 specimens, 1487 (17%) were positive in 16 days by MGIT 960 compared to only 536 (6%) in 48 days by conventional method. In total 91% of the clinical specimens were positive by MGIT during first two weeks of incubation [Graph 1 - [SUPPORTING:1] ]. In contrast, only 4% were positive by L.J during first two weeks and 79% of were positive between four to eight weeks. Recovery of M. tuberculosis complex from different clinical specimens by MGIT and L.J was evaluated in [Table - 3]. Among the respiratory specimens, of the 7823 specimens tested 4334 (55%) were positive for M. tuberculosis complex by MGIT whereas only 2648 (34%) were detected by L.J. In case of non-respiratory specimens, significant recovery of M. tuberculosis complex isolates was observed by MGIT especially from aspirates (38%), Pus (37%) and Fine Needle Aspiration Collection (FNAC) (33%), tissues and lymph nodes (26%), pleural fluid (22%) and CSF (14%). Evaluation of PNBA assay on MGIT 960 system was done by comparing results of 440 culture isolates (307 M. tuberculosis and 133 NTM) with in-house molecular methods [Table - 4]. Results were comparable in 433 cases whereas discrepancy was observed in seven cases. In two of the seven discrepant cases there was mixed infection with M. tuberculosis complex and NTMs and only NTMs were detected by PNBA. However, remaining five were falsely identified as NTMs. Overall sensitivity was 97% and specificity was 100%. Discussion MGIT 960 TB system incorporates an enriched Middle-brook 7H9 broth with patented sensors to make efficient use of an advanced fluorometric technology via detection of O 2 consumption. At our tertiary care centre, a statistically significant difference (p< 0.000001) in recovery rate was demonstrated by MGIT 960 TB system compared to conventional L.J method. The system was found to be more advantageous in paucibacillary specimens like CSF, body fluids, and FNAC, whereas L.J media yielded scanty or no growth. We observed that highly smear positive specimens (3+), a MGIT culture scored almost 99% recovery within 48-72 hours of culture inoculation. However, in case of smear negative specimens an average detection time was found to be 16 days compared to 48 days by L.J. method [Table - 2]. Amongst the total culture positive specimens (6143), 91% were detected by MGIT in first 2 weeks. In contrast L.J only 5% were detected by L.J in the first two weeks and 79% between three to eight weeks. Nearly 15% specimens were positive by L.J after eight weeks highlighting the importance of incubating L.J for a longer time (at least 10-12 weeks). In case of pulmonary specimens, the mean recovery time was 8.7 days where as in case of paucibacillary extra-pulmonary specimens it was found to be 13.2 days by the MGIT 960 TB system. Isolation and identification of M. tuberculosis complex using PNBA assay in the MGIT medium has been evaluated in a number of reports. [2],[3],[4],[5] In the present study, 100% concordance was observed between NAP and PNBA assay results. Further confirmation of PNBA results using in-house RLBH assay and sequencing [Table - 4] showed discrepancy in seven cases. All these seven isolates were also identified as NTM by NAP test. Of these, seven in two cases there was mixed infection and only NTM were detected by NAP/ PNBA. However, the remaining five were falsely identified as NTM. Various factors associated with false phenotypic identification include, error in inoculum size, growth phase of mycobacteria, concentration of NAP / PNBA per ml of the cultivation media, contamination due to any other gram positive and gram negative bacteria, NAP / PNBA resistant strains of M. tuberculosis complex etc. However, in the present study, retesting of all these five cases by both the methods did not show any change in the results. This false identification by the phenotypic methods could be due to the resistance of these 5 M. tuberculosis complex isolates to NAP / PNBA. All the 133 were confirmed by molecular methods and the results showed 100% concordance with PNBA and NAP results. The median time to obtain presumptive identification of M. tuberculosis complex by PNBA inhibition test in BACTEC 960 TB system was six days. In our experience, the PNBA assay compares well with NAP, and showed 97.6% sensitivity and 100% specificity against in-house RLBH assay and sequencing. Hence it can be adapted in the routine laboratory on all MGIT positive vials. However, it should be borne in mind that lateral flow assays as Capilia TB will further reduce the time for identification to 20 mins. [13],[14] Compared to our previous data using BACTEC 460 TB system, the lower rate of recovery was observed in smear negative clinical specimens (especially sputum) due to a higher contamination rate with the MGIT 960. [15] Of the total 14,597 specimens analysed, contamination rate in smear negative sputum specimens was found to be 4% using MGIT 960TB system. This could be because the MGIT 960 medium is rich in protein thereby growing contaminating organisms, which survived the decontamination process. The BACTEC 460 TB is comparatively low in nutrient content and only detects organisms that metabolize the [14] C labeled substrate Palmitic acid. Many contaminants do not metabolize this substrate. Studies published by Hanna et al , Tortoli et al , Leitritz et al , Williams Bouyer et al . and Whyte et al . reported higher contamination rate with MGIT 960 than that of BACTEC 460 TB system. [2],[4],[16],[17],[18] MGIT 960 requires careful processing and handling of specimens. In countries like ours, higher cost is a major limitation. MGIT 960 TB system involves high initial investment of nearly 3.5 million rupees and with a high recurring cost of 120 Rs (2.5 USD) per MGIT vial. In India, an average cost for isolation and identification using MGIT 960 TB systems is Rs. 500 (10 USD) per patient as compare to Rs. 50 (1 USD) using L.J. medium [Table - 5]. Further identification of MGIT positive culture isolates using commercial molecular methods like Accuprobe costs approximately 550 Rs. (11 USD) with a total cost Rs 1050 (21 USD) for culture and identification. In contrast, the PNBA assay on MGIT costs only Rs.550 (11 USD) for both culture and identification. In summary, the recently introduced fully automated 7 ml BACTEC MGIT system with PNBA assay for identification of M. tuberculosis complex is useful for laboratories processing a large number of specimens daily. The cost benefit should be evaluated in the context of rapid and effective patient management. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09064t3.jpg] [mb09064g1.jpg] [mb09064t2.jpg] [mb09064t4.jpg] [mb09064t5.jpg] [mb09064t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}