 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
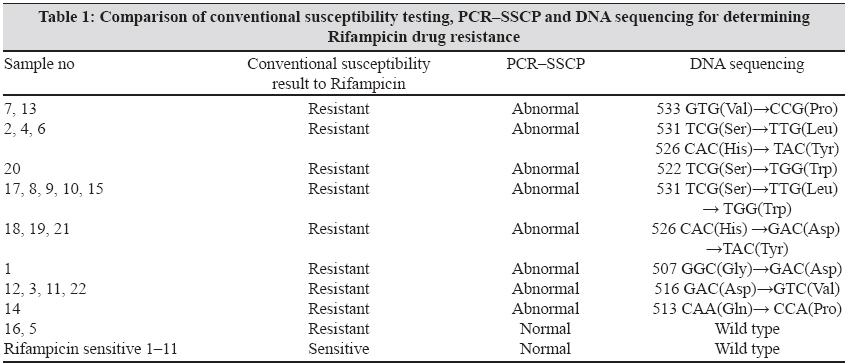
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 226-230 Original Article Characterization of RPO B gene for detection of rifampicin drug resistance by SSCP and sequence analysis Negi SS, Singh U, Gupta S, Khare S, Rai A, Lal S National Institute of Communicable Diseases, Ministry of Health and FW, Government of India, 22-Shamnath Marg, Delhi-110 054 Date of Submission: 10-Jul-2008 Code Number: mb09066 PMID: 19584503 Abstract Purpose: Because of the emergence of multidrug-resistant tuberculosis in recent times, the rapid detection of resistance to the first-line anti-tuberculosis drug rifampicin was felt worldwide. Accordingly, this study was conducted to evaluate the diagnostic potential of polymerase chain reaction-single strand conformation polymorphism (PCR-SSCP) for checking its utility as a rapid screening test for determination of rifampicin drug resistance.Materials and Methods: A total of 34 isolates of Mycobacterium tuberculosis ( M. tuberculosis ) (22 rifampicin resistant, 11 rifampicin sensitive and one control H37Rv) strains were analysed by PCR-SSCP and DNA sequencing within the 157-bp region of the rpo B gene (Ala 500 -Val 550 ). Results: Rifampicin resistance was detected successfully by PCR-SSCP in 20/22(90.90%) of rifampicin-resistant strains showing a total of nine different mutations in seven codon positions: codon 513 (CAA→CCA), 516 (GAC→GTC), 507 (GGC→GAC), 526 (CAC→GAC, TAC), 531 (TCG→TTG, TGG), 522 (TCG→TGG) and 533 (GTG→CCG). Two rifampicin-resistant strains showed an identical PCR-SSCP pattern with the wild type H37Rv; 77.27% rifampicin-resistant strains showed a single point mutation and 9.09% had no mutation. Three rifampicin-resistant strains showed characteristic double mutations at codon positions 526 and 531. Sensitivity and specificity were calculated as 90.90% and 100%. Conclusions: Rifampicin-resistant genotypes were mainly found in codon positions 516, 526 and 531. PCR-SSCP seems to be an efficacious method of predicting rifampicin resistance and substantially reduces the time required for susceptibility testing from 4 to 6 weeks to a few weeks. Keywords: M. tuberculosis, multidrug resistant tuberculosis, polymerase chain reaction-single strand conformation polymorphism Introduction The rapid detection of resistance to first-line drugs such as rifampicin is essential for the efficient control of multidrug-resistant tuberculosis (MDR-TB) as rifampicin resistance was found to be an important marker for checking MDR in clinical isolates of Mycobacterium tuberculosis. [1],[2] Although the period required for culturing is shortened by the BACTEC system, drug susceptibility testing in a liquid medium still requires 1-2 weeks for final reporting. Rifampicin-resistant strains of M . tuberculosis evolve due to mutation in the rpo B gene encoding the β-subunit of the DNA-dependent RNA polymerase.[3] The resistance in more than 95% of the resistant strains is due to missense mutation or, less commonly, small deletions or insertions within an 81 bp rifampicin resistance determining region of the rpo B gene corresponding to codon position 507- 533. [3] Various molecular methods have been applied to detect these unique mutations, including polymerase chain reaction (PCR)-mediated single strand conformation polymorphism (SSCP) analysis, line probe assay and DNA sequence analysis. [1],[4],[5],[6],[7],[8] PCR-SSCP analysis involves amplification by PCR of a segment of the gene encoding the specific drug target and comparison of PCR products of drug-sensitive and drug-resistant strains by SSCP in which mutations usually result in an altered pattern. [9] This technique is relatively simple and was promising initially, but recent studies have questioned its sensitivity and specificity. [10],[11] In this study, we investigated the usefulness of the PCR-SSCP method to detect mutations in the rpo B gene of rifampicin-resistant and rifampicin-sensitive M. tuberculosis strains isolated inthe year 2006. The results were compared with sequencing with an aim to determine the codon most frequently involved and with phenotypic drug susceptibility testing. Materials and Methods Thirty-three strains of M. tuberculosis (22 rifampicin resistant and 11 rifampicin sensitive), which were isolated at the Natinal Institute of Communicable Diseases using a conventional L-J media-based culture, were obtained from equal number of patients with active TB (strong clinical/radiological/histopathological evidence of TB) referred from different hospitals of Delhi, like Lok Naik Jai Prakash, Guru Teg Bahadur, Kalawati Saran Children, Rajan Babu TB hospital, in the year 2006. The sensitivity/resistance patterns of these isolates to rifampicin were determined by drug susceptibility testing by the proportion method using L-J media. [12] Briefly, the L-J medium with and without rifampicin (critical concentration 40μg/mL) was inoculated with 0.1mL of neat and 10−2 dilution of a McFarland 1.0 concentration of a suspension of each isolate of M. tuberculosis . The inoculated bottles were then incubated at 37° C for 6 weeks. Reading of the sensitivity pattern of the mycobacterial isolates was taken at 4 and 6 weeks. The break point was 1%, i.e., the isolate was considered susceptible to rifampicin if the number of colonies that grew on the drug containing media were < 1% of the number of colonies that grew on the rifampicin-free media. An isolate was considered resistant if 1% or more grew on the drug-containing bottle. The H37Rv strain of M. tuberculosis was used as positive control strain. DNA extraction PCR SSCP DNA sequencing Results PCR-SSCP was performed on 34 strains of M. tuberculosis (22 resistant, 11 sensitive and one control H37Rv) with a fact that two denatured strands of DNA (in this case PCR amplified) adopt stable intra molecular conformations that may differ from the wild type on mutation. This causes a change in the electrophoretic mobility of the strands. The results of SSCP analysis of rpo B amplicons are summarized in [Table - 1]. The results of SSCP analysis reveal that while most of the rifampicin-resistant strains exhibited mobility shifts correlating with point mutation, the finding of a three band SSCP pattern may reflect the presence of two possible conformations for one of the DNA strands or a reannealing band, but, in any case, it does not interfere with pattern recognition. [9] On the basis of the SSCP results, 22 rifampicin-resistant isolates revealed 10 types of different band patterns [Figure - 1]. Lanes 2-11 showed the SSCP pattern of the different resistant strains. All 11 rifampicin-sensitive strains had a PCR-SSCP pattern identical to H37Rv. Two rifampicin-resistant isolates had an PCR-SSCP pattern similar to that of the M. tuberculosis susceptible control strain H37Rv. DNA sequence analysis of 20 out of the 22 resistant strains revealed 10 different kinds of missense mutations affecting seven amino acids within a 81 bp region of the rpo B gene [Figure - 2]. Of the 22 sequences of rifampicin-resistant isolates, 17 strains showed a single mutation in the 81 bp core region and three strains showed double mutations at codon positions 531 ser and 526 His . Two rifampicin-resistant strains did not show any mutation/changed band pattern by either sequencing/SSCP. Highest frequency of mutation was observed in five rifampicin-resistant strains showing single point mutations at codon position 531 and four at codon position 516. Mutations were also found at codon positions 533, 522, 526, 507 and 513 by two, one, three, one and one strain, respectively. Discussion Rifampicin is known to be a fast-acting bactericidal agent against M. tuberculosis and has greatly shortened the duration of chemotherapy. [3] However, rifampicin-resistant or MDR M. tuberculosis strains have become a newly emerging problem. [3] Because rifampicin resistance can be regarded as a possible marker of MDR, application of a rapid DNA-based assay would be a convenient method for suggesting drug susceptibility patterns. [5],[16],[17] Rifampicin resistance has been attributed to point mutations in the rpo B gene rather than to acquisition of a transposable element by M. tuberculosis . The point mutations can be easily detected on DNA sequencing of the resistant strains. These mutations can also generate unique intra strand associations in the ssDNA of the resistant mutants, leading to conformational polymorphism. These conformational changes can cause mobility shifts on the gel resulting in an altered band pattern, which differentiates between sensitive and mutant strains. Keeping the above principle in mind, PCR-SSCP of 33 test isolates was carried out of which 11 were phenotypically predetermined to be sensitive and the remaining 22 were phenotypically resistant. We used an H37Rv rifampicin-sensitive strain as the control. Eleven phenotypically sensitive strains showed the same characteristics, three bands coinciding with the bands of the control strain at the same position thus showing a 100% positive result whereas the phenotypically resistant strains, sample nos. 1-20, exhibited a band position displacement suggesting conformational change due to mutation. The technique of PCR-SSCP is highly reproducible although it should be considered that differences in methods and protocols might produce a different banding pattern. Irrespective of local differences, our data also demonstrated that SSCP analysis is highly specific and sensitive for detecting mutations in the rpo B gene in rifampicin-resistant M. tuberculosis strains. The sensitivity/specificity of this method was 90.90%/100%. Thus, this method can be considered as a reliable method for detection of mutations responsible for conferring rifampicin resistance. The PCR-SSCP method detects only the presence and not the types of mutations. For this reason, PCR-SSCP analysis should be supported by DNA sequencing. In this study, the three strains (numbered 2, 4 and 6) showed double mutation, the first at codon position 526 His and the second at 531 Ser . The PCR-SSCP pattern of these strains was different from that of the strain with a mutation either only at Ser531 or His526 and from that of the one reference strain, H37Rv. In this study, two rifampicin-resistant isolates had a PCR-SSCP pattern similar to that of the M. tuberculosis -susceptible control strain H37Rv. These results may imply a mutation in another part of the rpo B gene or the existence of at least one additional gene that participates in rifampicin resistance. The sequencing result of this strain demonstrated no mutation in the 81 bp region. The mutation responsible for rifampicin resistance in this strain could be located either outside the region of analysis (such as codon 146) or changes that might have occurred in genes whose products participate in antibiotic permeation or metabolism. [3],[9],[18] This observation confirms an earlier report of a rifampicin-resistant strain identified in Australia with a mutation outside the core region of rpo B . [19] We compared our PCR-SSCP result with the earlier published data. Earlier studies also showed that rifampicin-resistant M. tuberculosis strains have shown missense mutation, easily detected by PCR-SSCP, in a highly conserved region of the rpo B gene encoding Leu 511-Leu 533. [1],[5],[9],[10],[11],[14],[16] Isfahani et al. [1] showed 95.2% sensitivity by PCR-SSCP for detection of mutations in the rpo B gene. However, on the basis of the SSCP result of Miriam et al. , [11] the 35 rifampicin-resistant isolates were grouped in to two main categories: group one, 24 isolates (68.6%) with an SSCP identical to that of the control strain H37Rv and group two, 11 isolates (31.4%) with an SSCP different from that of H37Rv. In their study, there were also 11 rifampicin-sensitive isolates that showed an SSCP identical to that of H37Rv. Lee et al. [10] assessed the molecular mechanisms of rifampicin resistance in clinical strains of M. tuberculosis . The molecular nature of a part of the rpo B gene in 77 M. tuberculosis clinical strains isolated in Korea was analysed using PCR-SSCP and PCR-sequence analysis. Among 67 rifampicin-resistant isolates, 50 showed SSCP profiles different from that of a rifampicin-sensitive control strain, M. tuberculosis H37Rv, whereas 17 resistant isolates displayed SSCP profiles indistinguishable from that of the sensitive control strain. This might be due to the presence of a mutation outside the amplicon. After sequencing of the 81 bp region of the rpo B gene of the 22 rifampicin-resistant isolates, 17 (77.2%) strains showed a single mutation. Upon analysis of mutation frequencies, a majority of the mutations were found at codon positions 531, 526 and 516, corroborating the statement that these mutation are the most prevalent worldwide. [1],[3],[4],[5] This finding is comparable with the results of earlier studies demonstrating the rpo B mutation in different geographic areas. [5],[6],[7],[9],[14] Another characteristic finding was that of the double mutation occurring in two separate codons 526 and531 in three rifampicin-resistant strains, which again suggests that mutations of these two amino acids are the most frequent and are critically related to rifampicin resistance. In summary, our data and earlier studies on rpo B mutation frequencies supported the common notion that rifampicin resistance genotypes with mutations at critical codons, i.e., those encoding Ser531, His526 and Asp516 were most frequently detected in M. tuberculosis , regardless of the geographic origin. We also analysed the cost issue parameter associated with the PCR-SSCP test. The currently available method for rifampicin drug resistance includes commercially available line probe assay (Inno-Li PA kit), mycobacteriophage-based assay, DNA sequencing and single tube heminested PCR assay. Each technique has its own drawbacks and advantages. [20] Although there are several advantages to the line probe assay, it is more expensive than the other methods and requires several probes for reverse hybridization to determine the mutation. Mycobacteriophage assay is still not standardized and thus not widely used. Heminested PCR uses signature nucleotides of M. tuberculosis to avoid amplification of DNA from other GC-rich bacteria. It is a powerful method to detect rpo B DNA of M. tuberculosis directly from sputum samples. However, when this method was applied to detect M. tuberculosis rifampicin resistance, further analysis such as sequencing or dideoxy fingerprinting after the amplification of the 193 bp rpo B DNA by heminested PCR was required. Sequencing is costlier than PCR-SSCP. Hence, because of the above said reasons, we found PCR-SSCP a better option for rapid and accurate detection of rifampicin resistance. The technique of PCR-SSCP could be applied to other targets such as detection of fluoroquinolone, pyrazinamide, streptomycin or ethambutol resistance. [17] Moreover, there is an ample opportunity for using PCR-SSCP directly on the clinical specimens. But the question is where and how these tests could be incorporated into routine use? Certainly there are settings where the rapid identification of drug resistance may be highly desirable and may prove to be cost effective. A primary example would be the urban population with a significant prevalence of MDR-TB and human immunodeficiency virus coinfection where data on the resistance genotype may result in better patient management and in more effective utilization of isolation rooms. However, we can say that although SSCP has a great advantage in reducing the time required for determination of sensitivity pattern from 6 weeks to 2-3 days, it is still limited by the requirement of extensive labour and a level of technical expertise not found in most clinical laboratories. Overall, we believe that use of PCR-SSPC for rifampicin resistance may result in a net time gain of several weeks over conventional resistance testing. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09066f2.jpg] [mb09066f1.jpg] [mb09066t1.jpg] |
| |||||||||
{kind=link}
{kind=link}