 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
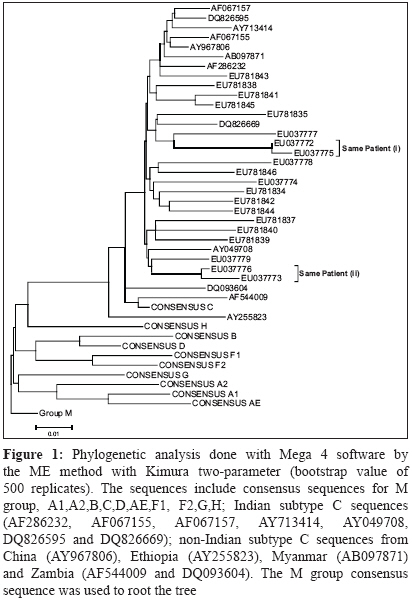
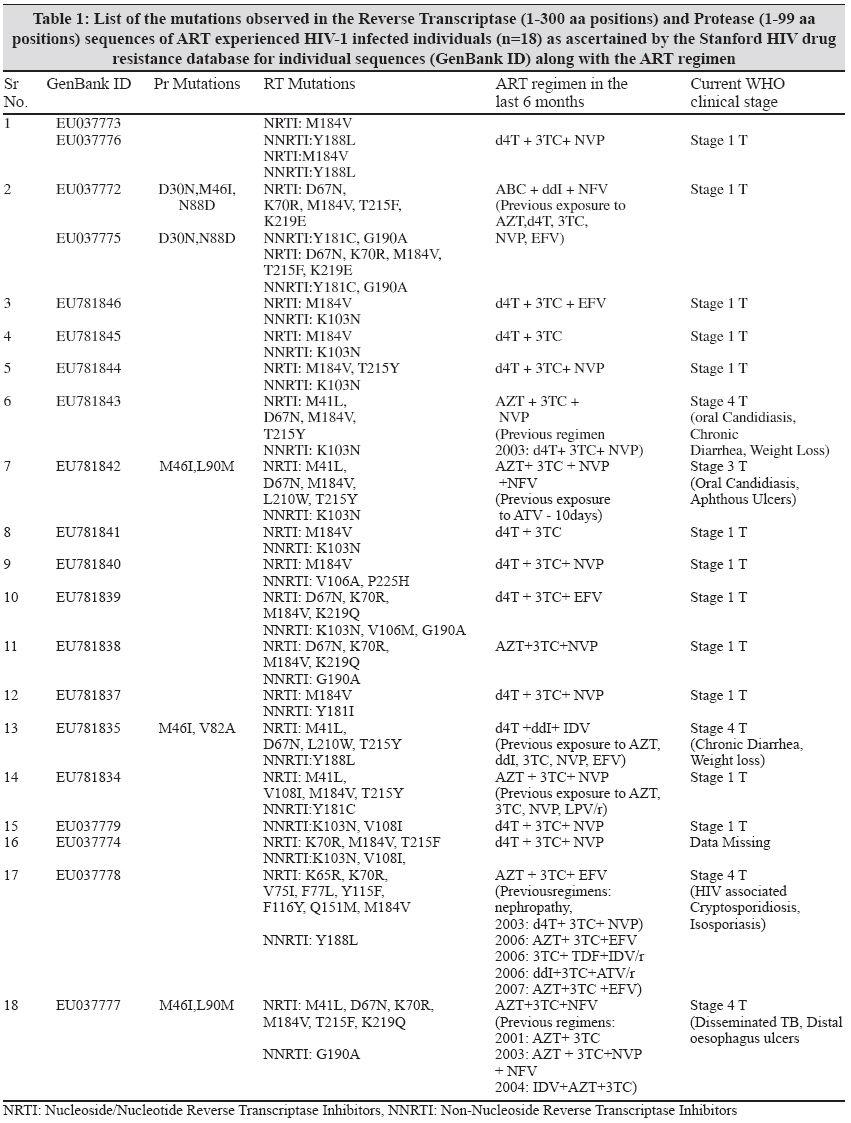
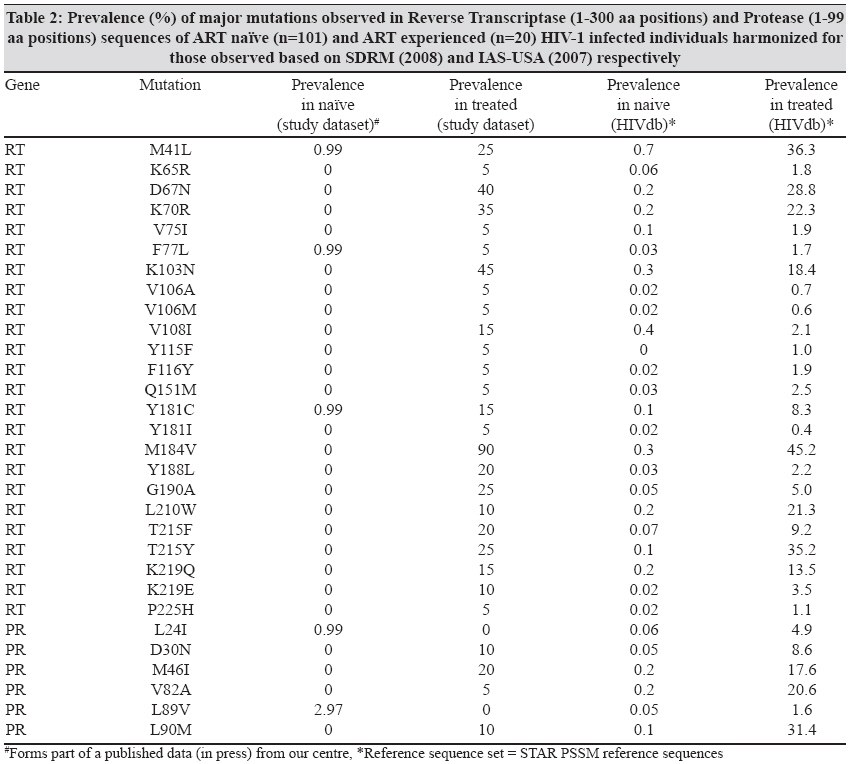
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 231-236 Original Article Drug resistant mutations detected by genotypic drug resistance testing in patients failing therapy in clade C HIV-1 infected individuals from India Kandathil AJ, Kannangai R, Verghese VP, Pulimood SA, Rupali P, Sridharan G, Grant P, Pillay D, Abraham OC Department of Internal Medicine, Christian Medical College, Vellore 632 004 Date of Submission: 22-Jan-2009 Code Number: mb09067 PMID: 19584504 Abstract Purpose: There has been an increase in the number of individuals administered antiretroviral therapy (ART) in India but treatment outcome is hampered by increasing development of drug resistance. Previous reports from India have shown M184V as the commonest mutation in treated individuals. However, there is no evidence for any protease mutations in these reports. This study was done to observe the common/unique mutational patterns observed in reverse transcriptase (RT) and protease (Pr) genes of clade C HIV-1 strains from individuals showing treatment failure in India.Materials and Methods: The assay was done by sequencing the Pr and RT genes of the HIV-1 strains from 18 individuals failing ART. Analysis was carried out using Stanford HIV drug resistance database (SHDB). The sequences were also submitted to the calibrated population resistance tool of SHDB and Rega HIV-1 sub typing tool. Phylogenetic analysis and quality control were performed with Mega 4. Results: Among the 20 strains, 19 showed resistance to both nucleoside reverse transcriptase inhibitors (NRTIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs), one strain to NNRTIs and five strains showed protease inhibitors (PI) resistance and 3-class resistance. The most common mutation conferring NRTI resistance was M184V (90%) while K103N (45%) was the most common mutation conferring NNRTI resistance. The M46I mutation was seen in 20% of the Pr sequences. Conclusion: Resistance testing to check the prevalence of drug resistance mutations that arise following failure of the first line regimen to establish guidelines for second line regimens in India is a must. Studies are needed to confirm if mutation patterns that arise among clade C following failure of ART are the same as for clade B strains. Keywords: Clade C, drug resistance, HIV-1, India, treatment failure Introduction There has been an increase in the number of individuals administered antiretroviral therapy (ART) in India under the auspices of the National AIDS Control Organization (NACO), India. ART is known to reduce morbidity and mortality associated with HIV infection but there are a number of factors that can hamper its benefits, with adherence being one of them. [1] Adherence is a dynamic process and can vary not only among HIV infected individuals but also in a given individual from time to time. [2] Individuals with a high level of adherence have a greater chance of viral suppression than individuals who are moderately adherent or non-adherent. [2] Incomplete suppression can lead to emergence of drug-resistant strains. [3] Previous reports from India have reported M184V as the most commonly observed mutation in the reverse transcriptase (RT) of HIV-1 strains in patients failing ART. [4],[5] This is a preliminary report based on findings of a study on drug resistant mutations that emerge in the RT and protease (Pr) genes of HIV-1 strains in infected individuals on ART in India. This report would contribute to the global data on the common mutational patterns observed in clade C HIV-1 strains from India available in the drug resistance database like the Stanford HIV database. Materials and Methods Blood samples were collected from 18 HIV-1 infected individuals at the clinical virology department of a tertiary care center in South India. These individuals were referred from the infectious disease clinic of the hospital for CD4+ T cell estimation and HIV-1 viral load testing. For this study, only individuals with detectable HIV-1 viral loads more than eight months after initiation of ART during the year 2005-2007 were recruited. Informed consent was obtained from all the individuals before collection of the samples. This study was approved by the Institution Review Board (IRB). Among the 18 treatment experienced patients, follow up information were available for two patients. The Guava ® Easy CD4T System (Guava Technologies, Hayward, CA, USA), as described earlier, was used for CD4 estimation. [6] Viral load estimation was done using Artus RealArtT HIV-1 kits (Qiagen Hamburg Gmbh, Germany) using Rotor- GeneT 3000. [7] The genotypic resistance assay was carried out by sequencing the Pr and RT genes. HIV-1 RNA was extracted from plasma using QIAamp ® viral RNA extraction kit (Qiagen GmbH, Hilden, Germany). Amplification and sequencing of the Pr and RT genes and was carried out as previously described. [8] All the sequences were also submitted to the calibrated population resistance tool (CPR) available at the Stanford HIV drug resistance database. Information on the frequency of mutations observed in our strains was generated based on the drug resistance mutation list of the IAS-USA major (2007). Phylogenetic analysis and quality control of sequences were performed for the 20 sequences with Mega 4 software using a minimum evolution method with Kimura two-parameter and bootstrap value of 500 replicates. [9] These were compared to the HIV-1 pol sequences obtained from the Los Alamos HIV sequence database. The sequences included were consensus sequences for M group, A1,A2,B,C,D,AE,F1,F2,G,H; Indian subtype C sequences (AF286232, AF067155, AF067157, AY713414, AY049708, DQ826595 and DQ826669), non-Indian subtype C sequences from China (AY967806), Ethiopia (AY255823), Myanmar (AB097871) and Zambia (AF544009 and DQ093604). The M group consensus sequence was used to root the tree. The sequences were also submitted to the Rega HIV-1 sub typing tool. [10] Results The mean HIV-1 viral load in this group was log 10 5.54 copies/ml with a median value of log 10 4.72 copies/ml. The CD4 counts available on 16 patients ranged from 26 - 1155 cells/mm 3 , with a median value of 306 cells/mm 3 and mean of 313 cells/mm 3 . Among the 18 patients who had an age of range of 11-47 years there were 15 (83%) males and three (17%) females. The study population consisted of individuals from South (n=16, 89%), East (n=1, 5.5%) and North (n=1, 5.5%) India. In the phylogenetic tree [Figure - 1] the study sequences were individually distinct and seen to segregate with consensus C at the major node indicating robust sequencing information. Similar results were obtained using the REGA HIV-1 Sub typing Tool - v2.0. Among the 20 strains, 19 showed resistance to both nucleoside reverse transcriptase inhibitors (NRTIs) and non-nucleoside reverse transcriptase inhibitors (NNRTIs) while one strain was resistant only to the NNRTIs. Among the 20 strains, five strains were resistant to protease inhibitors (PIs). These five strains showed three-class resistance i.e., they were resistant to NRTIs, NNRTIs and PIs. The RT gene showed major mutations at 20 sites with 24 mutation patterns while the Pr gene showed 4 mutation patterns at 4 sites. The combination of mutations observed in the RT and PR sequences along with the ART combinations are shown in [Table - 1]. Amplification and sequencing of the reverse transcriptase gene revealed eighteen (90%) strains with M184V substitution, a known 3TC resistance-conferring mutation. Among the observed substitutions, K103N, Y181C, Y188L and G190A have implications for NNRTI resistance while M41L, D67N, K70R, T215F and T215Y have been implicated in NRTI resistance. The most common substitution responsible for resistance to PIs was M46I (n=4) in these strains. The other substitutions observed were D30N and L90M (n=2, each). The prevalence of major amino acid substitutions seen in RT and Pr known to affect susceptibility to the different classes of drugs used in ART are shown in [Table - 2]. The difference in the prevalence of the mutations between the study sequences and the Stanford database is shown in [Table - 2]. Discussion The RT amino acid sequence was found to have more drug resistance-conferring mutations than the Pr amino acid sequence. This could be explained as the outcome of all patients having received at least one regimen containing NRTIs plus NNRTIs. PI mutations were seen in only 4 of 18 patients, as PI use is still limited in India. Eighteen (90%) of the 19 strains sequenced in this group had the M184V mutation. This mutation is selected for by lamividune (3TC), emtricitabine (FTC) or abacavir (ABC) use and confers high-level resistance to 3TC. [11] Patients receiving incompletely suppressive 3TC regimens usually develop M184V as their first mutation. [11] The other mutations observed included nucleotide excision mutations (NEM) 41, 67, 70, 210, 215 and 219. [12] The most commonly occurring NEM was at position 215. The T215Y mutation was observed in 25% of the sequences while T215F was seen in 20%. These NEMs cause drastic reduction in susceptibility to azidothymidine (AZT). They do not, however, drastically affect the action of 3TC although they can affect the synergism of 3TC along with AZT. [11] Only 5% of sequences showed the Q151M mutation. The strain showing the Q151M substitution did not show any of the thymidine analogue mutations (TAMs) except for K70R; this strain also showed secondary mutations at positions 75, 77 and 116. The Q151M mutation is seen in patients receiving didanosine (ddI) in combination with AZT and stavudine (d4T) and is rarely seen in 3TC-containing NRTI regimens. [13],[14] As most first line ART regimens in India contain 3TC this may explain the low prevalence of Q151M in the study sequences. Previous publications from India have highlighted the absence or low prevalence of the Q151M mutation. [4],[5] Based on data from the West from previously published studies, M184V was the most commonly observed mutation in patients on NRTIs. [9] We have very limited data but the mutational patterns observed appear similar to published data. [4],[5],[11] One of the worrying factors is a recent report from western India which documented M41L, D67N, M184V, and A98G in the RT gene of treatment naοve individuals. [15] Mutations conferring resistance to NNRTIs were also seen, with one strain showing resistance only to NNRTIs. The NNRTI resistance-conferring mutations included K103N (45%), Y181C (15%) and Y188L (20%). Additionally, Y181I mutation conferring resistance to NNRTIs was seen in 5%. The minor mutations observed in the RT conferring resistance to NNRTIs that were observed included V90I, K101E and V106I. We were unable to discern any identifiable pattern of association between the major and minor mutations. Furthermore, the RT mutations were not restricted to any particular site domain of the RT molecule relative to its function. Four patients showed resistance to PIs. With the exception of L90M, the other mutations were observed near or in the flap region of the protease as deduced from 3D modeling. The flaps must be flexible in order to allow movement of the substrate and product. [16] D30N was observed in one of the patients showing failure to PIs. D30N confers resistance only to NFV with no cross-resistance to other PIs. [12] The patient who had the D30N mutation also had M46I mutation that was, however, not observed in the sequence of the sample sequenced at a second visit two years later. This could be indicative of reduced viral fitness of the strain, indirectly indicated by a reduced viral load with a log 10 0.43 reductions at the patient′s second visit. An alternative explanation could be amplification of a different quasispecies in the second sample. The M46I mutation contributes to reduced susceptibility to nelfinavir and fosamprenavir. [17] The N88D mutation was seen at both visits. L90M mutation was observed in two sequences and was present along with M46I. L90M has been reported from patients treated with saquinavir, nelfinavir, indinavir and ritonavir. [12] L90M has been implicated in clinical cross-resistance to each of the PIs. [12] In India, PIs are not normally part of first line antiretroviral regimens because of their cost. The low prevalence of protease mutations are similar to previously published literature from India among treatment experienced patients. [18],[19] The L89V mutation was seen in our treatment naοve population. In a recent study from western India among treatment naοve individuals has documented V82A mutation in the protease gene. [15] Based on the Stanford drug resistance database the mutation contributes to resistance to darunavir (DRV), which is however not used in ART regimens in India. This may possibly explain the lack of selection of this mutation in our treatment-experienced group. Based on data obtained from the Stanford HIV genotypic drug resistance database all the submitted sequences belonged to clade C. This was also supplemented with phenotypic analysis and results obtained from the REGA HIV-1 sub typing tool. This is consistent with genotypic data for strains from different regions of India including the south that have shown the predominant subtype to be clade C. [20] Prevalence (%) of major mutations observed in Reverse Transcriptase (1-300 aa positions) and Protease (1-99 aa positions) sequences of ART naοve (n=101) and ART experienced (n=20) HIV-1 infected individuals were harmonized for those observed based on SDRM (2008) and IAS-USA (2007) respectively. The RT amino acid sequence in the treatment-experienced group in our study had a higher prevalence of D67N, K103N, M184V and G190A than those seen in the HIV drug resistance Stanford database. This may be an outcome of the first-line ART regimen (two NRTIs and one NNRTI) followed in India. Based on our findings, we suggest the use of resistance testing to check the prevalence of the drug resistance mutation that arises following failure of the first line regimen. This will help in establishing guidelines for second line regimens in India. Further studies are needed to confirm if mutation patterns that arise following failure of therapy for clade C are the same for clade B strains. Acknowledgement We would like to thank the Christian Medical College Fluid Research for the partial funding for this study. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09067f1.jpg] [mb09067t2.jpg] [mb09067t1.jpg] |
| |||||||||

{kind=link}
{kind=link}
{kind=link}