 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
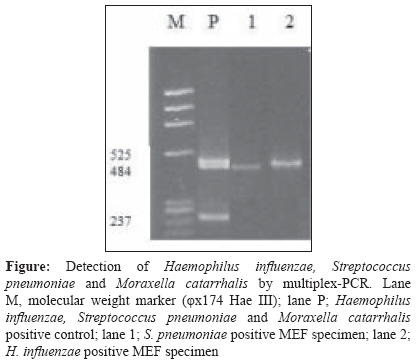
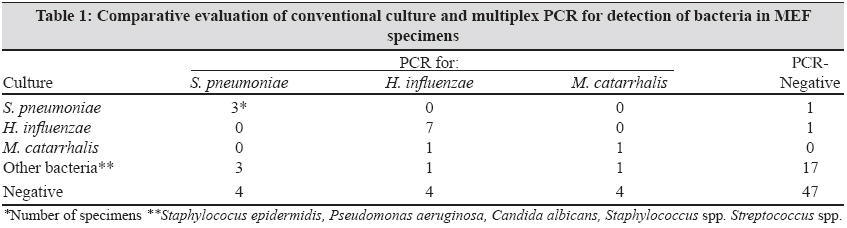
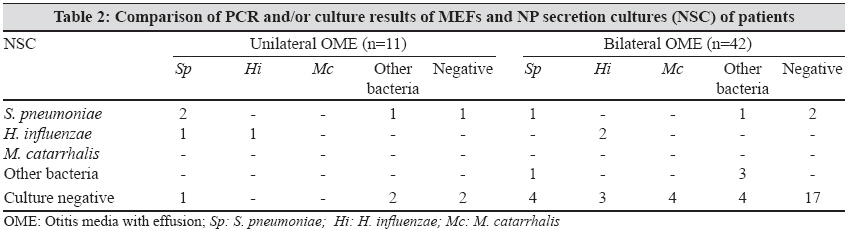
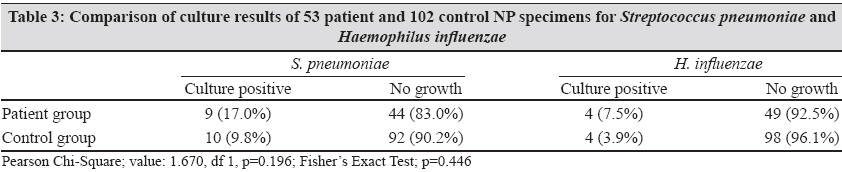
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 237-241 Original Article Efficacy of nasopharyngeal culture in identification of pathogens in middle ear fluid in chronic otitis media with effusion Eser OK, Ipci K, Alp S, Akyol U, Unal OF, Hascelik G, Sennaroglu L, Gur D Department of Microbiology and Clinical Microbiology, Hacettepe University, Ankara Date of Submission: 15-Dec-2008 Code Number: mb09068 PMID: 19584505 Abstract Purpose: Chronic otitis media with effusion (OME) is the leading cause of hearing loss during childhood. In bacterial etiology of OME, the most frequent pathogens responsible are Haemophilus influenzae followed by Streptococcus pneumoniae and Moraxella catarrhalis . This study aimed at evaluating the accuracy of nasopharyngeal (NP) specimens in the identification of pathogens in the middle ear fluid (MEF) in patients with OME.Materials and Methods: In this cross sectional, case-control study, 95 MEFs and 53 NP secretion specimens were obtained from 53 children. As a control group, 102 NP specimens were taken from children having an operation other than an otological disease. Conventional culture methods and multiplex-PCR method have been used to determine the etiology of OME; NP carriage between cases and control groups were compared using conventional culture methods. Pearson Chi-Square and Fisher's Exact tests were used in statistical analysis. Results : Bacteria were isolated by culture in 37.9% of MEF specimens, 14.7% of which belonged to the group H. influenzae , S. pneumoniae and M. catarrhalis. PCR was positive in 30.5% specimens targeting the same pathogens. There was a two-fold increase in carriage rate of S. pneumoniae and H. influenzae in patients than controls for each pathogen. Conclusion: PCR is a more reliable method to detect middle ear pathogens in MEF in comparison with the conventional culture methods. The NP colonization wasn't found to be an indicator of the pathogen in MEF although middle ear pathogens colonize more in nasopharynx of diseased children. Keywords: Chronic otitis media with effusion, Haemophilus influenzae, multiplex-PCR, Moraxella catarrhalis, Streptococcus pneumoniae Introduction Chronic otitis media with effusion (OME) is the most common cause of childhood hearing loss and can result in developmental impairment of linguistic, behavioural, motor and social skills. [1],[2],[3] OME has a multifactorial etiology like obstruction of eustachian tube, formation of biofilms, effect of allergens, extra-esophageal reflux and bacterial infections. Haemophilus influenzae, Streptococcus pneumoniae and Moraxella catarrhalis are the most common pathogens found responsible for bacterial infections in OME etiology. [3],[4],[5],[6] As frequency of identification of these agents by conventional culture methods is very low, in chronic OME, polymerase chain reaction (PCR)-based methods have been developed to increase their detection. [7],[8],[9] If nasopharyngeal (NP) culture can accurately identify middle ear fluid (MEF) pathogens, it will be a safer, inexpensive and less invasive technique than current assessment procedures. It will also allow physicians to make more timely management decisions for chronic otitis media patients. This study was carried out to evaluate the accuracy of NP specimens in the identification of pathogens in the MEF and compare the culture and multiplex-PCR methods in the detection of pathogens in MEFs of children with OME. The study was undertaken to compare NP carriage prevalence between chronic otitis media patient and control groups. Material and Methods Patients and specimens This study, designed as a prospective, hospital-based one, was in cross-sectional design to evaluate accuracy of NP isolates in identifying MEF pathogens and in case-control design to estimate the prevalence of NP carriage in chronic otitis media patients and controls. The study included 53 patients diagnosed with OME in a university hospital between January 1-June 30, 2006. All patients with chronic otitis media during the study period were selected. There were 53 NP secretions and 95 MEFs taken from these patients, 42 of whom provided two samples from both ears. Exclusion criteria were acute febrile illness, acute otitis media, respiratory tract infection and antibiotic therapy during the previous two weeks. As a control group, 102 NP secretion specimens were taken from children undergoing an operation with no otologic indication. These children were outpatients of ear, nose, throat (ENT) unit with a diagnosis of non-infectious, non-cancer illness. The MEF was collected during ventilation tube replacement. The specimen used for bacteriological culture was sent to microbiology laboratory in half-an-hour after its collection in a "Bactec Peds Plus (BD, Sparks, MD, USA)" culture bottle. The specimen used for molecular methods was stored immediately at minus 20°C until it was processed for DNA extraction. Multiplex-PCR analysis and culture methods were done in a blinded manner on all specimens. Culture of specimens Multiplex-PCR Statistics Results A total of 95 MEFs and 53 NP secretion specimens were obtained from 53 patients between one and 12 years (mean age, 5.7). There were 31 males and 22 females in the group. A total of 102 NP secretion specimens were taken from 102 children as a control group. They were in the same age group with the patients (mean age, 5.2) and 61 of them were male, 41 female. Three main pathogens were isolated in 14.7% of patients by using conventional culture methods. H. influenzae, S. pneumoniae and M. catarrhalis was detected in 8.4%, 4.2% and 2.1% of patients, respectively. Other microorganisms such as Staphylococcus epidermidis, Staphylococcus warneri, Staphylococcus auricularis, alpha-hemolytic streptococcus, Pseudomonas aeruginosa and Candida albicans were detected in 22 patients. Multiplex-PCR was positive for one of the main three pathogens in 30.5% of MEFs. Each detected bacteria was classified as follows: H. influenzae in 13.7%, S. pneumoniae in 10.5% and M. catarrhalis in 6.3% of patients. No mixed bacterial DNA was found in any of MEF specimens. Positive PCR results of MEF specimens were shown in [Figure - 1]. Multiplex-PCR was positive for one of the pathogens in 12 culture negative specimens. Multiplex-PCR was also found positive in five MEFs having a positive culture for the other pathogens. Only two specimens were multiplex-PCR negative although one of them was positive for S. pneumoniae and the other for H. influenzae in bacterial culture. The comparison of bacterial culture and multiplex-PCR results is shown in [Table - 1]. Bilateral OME was seen as the most common pathology in 42 (79.2%) patients and unilateral OME was detected in 11 (20.8%) patients. Ten of the bilateral OME patients were positive for the same pathogen in both ears with either culture or PCR method. A comparison of the culture findings of NP secretion specimens and results of MEF, including both methods in 53 patients, show that six patients harboured the same species of bacteria both in NP secretion and one of their MEFs; three for S. pneumoniae and three for H. influenzae . In addition, six patients for S. pneumoniae , three for H.influenzae and four for M. catarrhalis were found positive in one of their MEFs although they were negative for the same pathogens in nasopharyngeal secretion cultures. On the other hand, three patients carrying S. pneumoniae in their NP flora were not found to be infected with the same organism in their MEFs [Table - 2]. When the NP secretion cultures of patient and control groups were compared, there was an approximately two-fold increase in carriage rate of S. pneumoniae and H. influenzae in patients than in controls for each pathogen but the detection rate did not show a statistically significant difference ( P =0.19 for Sp and P =0.44 for Hi) [Table - 3]. Discussion The three most commonly encountered pathogens playing a role in etiopathogenesis of OME are H. influenzae, S. pneumoniae and M. catarrhalis. This study confirmed the previous knowledge that H. influenzae, S. pneumoniae and M. catarrhalis are the most frequent microorganisms isolated from MEFs. [10],[11],[12] In this study, H. influenzae was found in the higher prevalence followed by S. pneumoniae in conventional culture method. On the other hand, coagulase negative staphylococci and Streptococcus spp, which colonize nasopharynx during childhood, were also in high prevalence. Although there are many studies demonstrating metabolically active bacteria in MEFs, identification of middle ear pathogens by conventional culture methods is not satisfactorily high in chronic OME. [6],[13] The detection rate of middle ear pathogens in MEF, with conventional culture methods, varies between 2-20% for these bacteria. [11],[12] According to this study, the detection rates for H. influenzae (8.4%), S. pneumonia e (4.2%) and M. catarrhalis (2.1%) were similar to other studies. Therefore, PCR-based methods are more reliable in the detection of these organisms. Multiplex-PCR method helps to improve the detection rate of these bacteria with respect to the conventional culture method. [8] In the present study, multiplex-PCR method had a better performance than conventional culture method in detecting middle ear pathogens in the analysed MEFs (14.7% versus 30.5%, respectively). The sensitivity of conventional culture methods decreases as the transportation of the specimen delays. They are time-consuming, labor-intensive and need experience in microbiological diagnosis. Thus multiplex-PCR, being a one step rapid method, might be considered as a routine diagnostic method in patients with OME. The NP culture in young children shows that M. catarrhalis, S. pneumoniae and H. influenzae are more likely colonized in the nasopharynx of children. [14],[15] Although these three pathogens are part of normal NP flora, an increased rate of colonization with these pathogens also increases the risk of acute and chronic otitis media. Chronic OME being associated with certain pathogen detection in the nasopharynx of children indicates a role of these bacteria in its etiology. [16],[17] In the present study, middle ear pathogens, S. pneumoniae and H. influenzae , colonized almost two times more in nasopharynx of the patients with OME than in control groups, although carriage of these bacteria in nasopharynx was not statistically significantly different in two groups. Frequent administration of antimicrobial agents can influence the composition of the nasopharyngeal bacterial flora. [18] This may interfere the dominance of alpha-streptococcal strains in respiratory tract flora which are important organisms in bacterial interference. [19] The NP flora of otitis-prone children contains less aerobic and anaerobic organisms but more respiratory pathogens. [20] In this study, none of 53 chronic OME children showed a predominance of alpha-streptococcus colonization in nasopharynx. As the colonization of middle ear pathogens is high in children with chronic OME, the use of nasopharyngeal cultures may be employed as an alternative method to identify middle ear pathogens. In this study, only six patients harbored the same species, both in their nasopharynx and MEFs. Our data showed the similar results with Clary et al . that nasopharyngeal culture can not be an appropriate clinical sample to identify the pathogens of chronic OME. [21] The data looked into showed that middle ear pathogens are still the most common bacteria in OME. The study suggests that in clinical practice multiplex-PCR may be considered a more useful rapid method in the diagnosis of OME etiology than the conventional culture method. It might still be suggested that further studies to provide more sensitive results for the diagnosis of middle ear pathogens in children with chronic OME using other PCR-based methods such as real-time PCR are needed. It is also necessary to keep in mind that PCR methods, especially in-house, have potential limitations like contamination, right selection of primer sequences, etc. The NP culture has not been considered a useful predictor of chronic OME in clinical practice since detection of culturable pathogens in samples of patients with chronic OME is low and it does not indicate the organism in MEF. Acknowledgments This study was presented at the 47th Annual Inter-Science Conference on Anti-microbial Agents and Chemotherapy (ICAAC), Chicago, September 17-20, 2007. This study was supported by a grant from Hacettepe University Scientific Researches Unit, Ankara, Turkey (Project no: 0302101003).References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09068t1.jpg] [mb09068t3.jpg] [mb09068f1.jpg] [mb09068t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}