 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
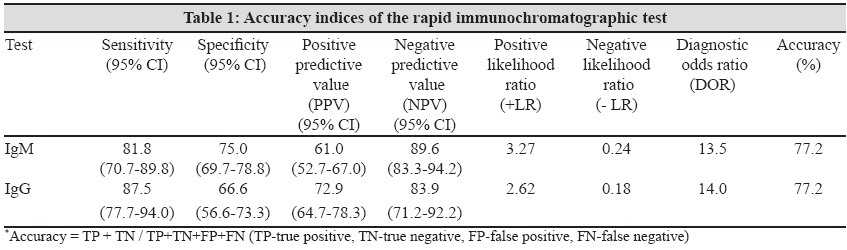
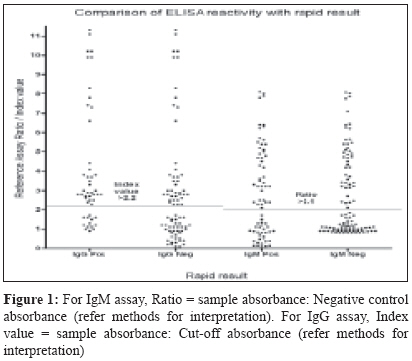
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 254-256 Brief Communication Evaluation of a rapid immunochromatographic device for the detection of IgM & IgG antibodies to Dengue viruses (DENV) in a tertiary care hospital in South India Moorthy M, Chandy S, Selvaraj K, Abraham AM Department of Clinical Virology, Christian Medical College, Vellore, Tamil Nadu - 632 004 Date of Submission: 17-Nov-2008 Code Number: mb09072 PMID: 19584509 Abstract This study has evaluated the performance of a rapid immunochromatographic test (ICT) device in detecting antibodies to Dengue virus (DENV) in a tertiary hospital in South India. Sera from hospital attendees, with requests for DENV antibody testing, were tested with the Panbio Dengue Duo Cassette and a reference antibody capture assay for the detection of IgM (Dengue IgM capture ELISA-National Institute of Virology, India) and IgG (Dengue IgG capture ELISA-Panbio Diagnostics Inc., Australia) antibodies. The ICT results were compared with results of antibody capture tests for the detection of the IgM and IgG antibodies, respectively. Accuracy indices for IgM and IgG detection, respectively were - sensitivity 81.8% and 87.5%, specificity 75.0%, and 66.6%, positive predictive value (PPV) 61.0% and 72.9% and negative predictive value (NPV) 89.6% and 83.9%. The device performs poorly in detection of IgM and IgG antibodies to DENVs and is not recommended for use as a stand-alone diagnostic test. Keywords: Antibody, dengue, immunochromatography Introduction Dengue is an acute febrile illness endemic to the Indian sub-continent. [1],[2] It is caused by dengue virus (DENV) - an arthropod-borne virus of the family Flaviviridae . Four distinct serotypes have been described for DENV - serotypes 1-4. [3] Primary DENV infections present as either a non-specific illness or dengue fever (DF). Secondary infection with a serotype different from that causing primary infection may lead to dengue haemorrhagic fever (DHF) or dengue shock syndrome (DSS). [4] The diagnosis of primary dengue is made by detection of IgM anti-DENV antibodies which appear 5-7 days after the onset of illness and persist for 2-3 months. Secondary infection is characterized by the production of IgG antibodies and a weak IgM response. This study was carried out to evaluate the performance of a rapid immunochromatographic test (ICT) device (Dengue Duo Cassette - Panbio Diagnostics Inc., Australia) for the detection of IgM and IgG antibodies to DENV at a tertiary care hospital in south India.Materials and Methods Serum samples from patients presenting to the hospital with dengue-like illness and for whom DENV antibody testing was requested between April 2006 and September 2007, were included in this retrospective evaluation. Samples were included in the study solely based on antibody reactivity and delinked from patients before inclusion. Sera whose rapid reactivity was known were included into one of the two panels based on the result of rapid testing. A panel of 138 serum samples (referred to as panel I) was selected for testing with the reference IgM assay (Dengue IgM capture ELISA - National Institute of Virology, India) to evaluate IgM detection . For the evaluation of IgG detection, a total of 86 samples (referred to as panel II) were tested with a reference IgG assay (Dengue IgG capture ELISA - Panbio Diagnostics Inc., Australia). The results of the rapid test were compared with that of the corresponding reference test (either IgM or IgG capture) and the accuracy indices of test performance were calculated. Dengue Duo Cassette: This device is based on the immunochromatographic principle that allows for detection of both IgG and IgM in a single test. Positive samples produce a pink line at the control and IgM or IgG position. Negative sample produce a pink line only at the control position. The assay was performed according to manufacturer′s instructions and results recorded independently by 2 persons and validated by a supervisor. A positive control was tested along with the samples. Dengue IgM antibody capture ELISA: This test detects DENV-specific IgM antibodies in an ELISA format. Kit controls and samples in duplicate were tested as per manufacturer′s instructions. [5] Samples were declared reactive based on the ratio of absorbance of sample to negative control. Positive samples showed a ratio greater than or equal to 2.1 while negative samples showed a ratio less than or equal to 1.9 and ratios greater than 1.9 but less than 2.1 were considered indeterminate. Dengue IgG capture ELISA: This test detected DENV-specific IgG antibodies. Appropriate controls (positive, negative and calibrator) along with sera in duplicate were tested as per manufacturer′s instructions. Samples were considered positive if the index value (ratio of sample absorbance to cut-off absorbance) was greater than 2.2 and negative if less than 1.8. Samples with index value between 1.8 and 2.2 were considered equivocal. Absorbance ratios for the IgM and IgG reference assays were entered into a database using Microsoft Excel and accuracy indices were calculated using SPSS version 12 (SPSS Inc., USA). Results A total of 138 serum samples of panel 1 were tested for the presence of DENV-specific IgM antibodies with the IgM capture assay. Of these samples, two showed an indeterminate result and were excluded from further analysis. The accuracy indices of the rapid device for the detection of IgM antibodies to Dengue virus were calculated and this is depicted in [Table - 1]. A total of 86 samples in panel 2 were tested for DENV-specific IgG antibodies by the IgG capture assay. Of these, seven samples showed an equivocal result and were excluded from further analysis. The accuracy indices of the rapid device for the detection of IgG antibodies when compared to the IgG capture assay for the detection of IgG antibodies are depicted in [Table - 1]. The sensitivity for detection of IgM and IgG is 81.8% and 87.5% respectively. The specificity for the detection of IgM and IgG are 75% and 66.6%, respectively. IgM detection (61.0%) has a lower positive predictive value than for IgG detection (72.9%). The negative predictive value for both IgM and IgG detection are moderate (89.6% and 83.9% respectively). The absorbance ratios of the reference assays in comparison with the rapid result are indicated in [Figure - 1].Discussion Dengue viruses have been isolated in India as early as the 1960s. [6] Dengue has become an emerging disease of concern in Tamilnadu [7] and other parts of the country where outbreaks of DF or DHF have occurred. [2],[8],[9] This study was embarked upon to determine the utility of a rapid device in the detection of DENV antibodies in a tertiary care setting. Numerous studies have been performed to evaluate rapid ICT for the detection of IgM and IgG antibodies to DENV with variable results. In general, performance of rapid devices improved between acute and convalescent sera and drawing of paired blood samples is suggested to improve accuracy of diagnosis. [10] IgM detection between acute and convalescent sera, showed minimal improvement in sensitivity as compared to a marked improvement in specificity. [11] Also, higher rates of positivity was reported in patients with Flavivirus infections, probably indicating cross reactivity with other viruses, especially Japanese encephalitis (JE). [12] Experience from our centre showed a better sensitivity for an IgM capture assay compared to a rapid device. [5] In this study, detection of IgM as compared to IgG had poorer sensitivity, but higher specificity. For both IgM and IgG detection, the likelihood ratios were not high enough to be recommended as a good diagnostic test. The device may be used as a screening assay that would need to be confirmed with an antibody capture assay. The rapid device tested and evaluated has the ability to detect and discriminate both IgM and IgG antibodies in a sample. Testing with the device is relatively easy to perform, and interpretation of results unambiguous, though inter-observer variation is rarely seen. A few drawbacks of this study are noteworthy: 1) Samples declared as equivocal by reference assays were excluded from analysis during the calculation of accuracy indices. The design of the study prevented us from obtaining a repeat sample for testing. 2) Clinical data along with laboratory data would have provided a clearer picture of the performance of the device. Clinical data was not available as delinked samples were used for this evaluation. 3) In the panel included for the evaluation, only 1 assay (IgM or IgG capture ELISA) was used to classify DENV infection in patients. It is likely that some antibody negative samples may have been positive by antigen detection, culture or RT-PCR, if it had been attempted. 4) The DENV IgM as well as IgG antibodies show some cross reactivity with other members of the Flaviviridae family. This can lead to an over-estimation of infection rates especially during secondary infection. Tests for the detection of other Flavivirus infections were not done nor were samples representative of these infections included in the serum panels. Considering its moderate performance, we recommend that this device not be used as a stand-alone test, but that it is supplemented with another reference assay for diagnosis of DENV infection. As Dengue has already emerged as a significant problem in our country, further population-based studies are needed to evaluate the performance of the device. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09072t1.jpg] [mb09072f1.jpg] |
| |||||||||
{kind=link}
{kind=link}