 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
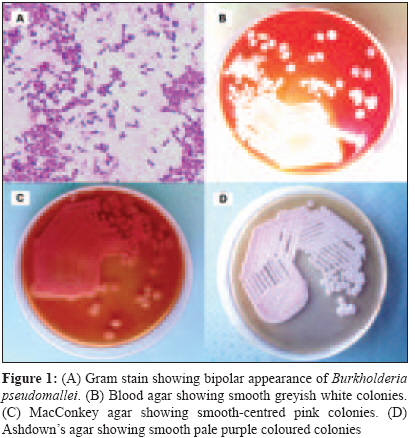
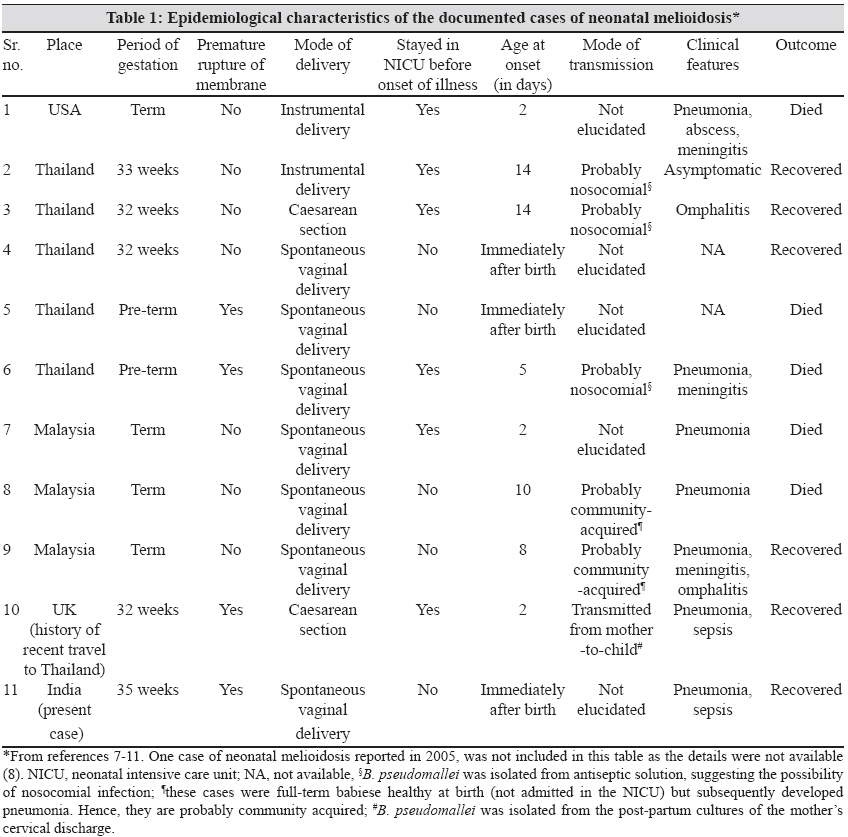
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 260-263 Case Report Neonatal melioidosis: A case report from India Noyal MJC, Harish BN, Bhat V, Parija SC Department of Microbiology, Jawaharlal Institute of Post-Graduate Medical Education and Research (JIPMER), Pondicherry 605 006 Date of Submission: 17-Nov-2008 Code Number: mb09075 PMID: 19584512 Abstract Melioidosis, caused by Burkholderia pseudomallei , is an infectious disease of major public health importance in Southeast Asia and Australia. We report, for the first time from the Indian subcontinent, a case of melioidosis in a neonate, its clinical presentation, microbiological diagnosis, possible mode of transmission and outcome. A pre-term female baby developed respiratory distress soon after birth. The child was febrile, had tachypnea, grunting, normal heart rate with a low pulse volume and poor peripheral perfusion. Chest X-ray revealed right-sided bronchopneumonia. B. pseudomallei was isolated from the blood culture of the neonate collected aseptically. The neonate was successfully treated with meropenem.Keywords: Burkholderia pseudomallei, neonatal melioidosis, sepsis Melioidosis, caused by Burkholderia pseudomallei , is an infectious disease of major public health importance in Southeast Asia and Australia. [1] The clinical spectrum of B. pseudomallei infection is broad, ranging from an asymptomatic, sub-clinical infection or focal infection (localized abscess) to disseminated infection. [2] Because of the highly varied clinical presentation, lack of suspicion and poor access to health facilities by the rural population, melioidosis is largely underreported in India. Melioidosis is an uncommon cause of Gram-negative septicaemia in neonates. We report, for the first time from the Indian subcontinent, a case of melioidosis in a neonate, its clinical presentation, microbiological diagnosis, possible mode of transmission and outcome. Case Report A pre-term female baby (35 weeks), appropriate for gestational age, born by spontaneous vaginal delivery to a booked and immunized mother, developed respiratory distress soon after birth. Pre-natal history was normal and mother had no infections, medications or trauma during pregnancy. There was a history of spontaneous pre-mature rupture of membranes. The neonate′s Apgar scores were 7 and 8 at 1 and 5 min, respectively, and she weighed 1.9 kg at birth. On examination, the child was febrile (38.6 o C), had grunting and was lethargic. She had a respiratory rate of 68/min, rapid heart rate with a low pulse volume and poor peripheral perfusion. The child was provisionally diagnosed to have pneumonia with sepsis and was shifted to the Neonatal Intensive Care Unit (NICU) for respiratory support, pre-term care and monitoring. Laboratory investigations revealed leukopaenia (total leukocyte count 4500 x10 3 /µl), normal blood glucose, electrolytes and liver and renal function tests. The neonatal erythrocyte sedimentation rate was normal. Chest X-ray revealed right-sided bronchopneumonia. The neonate was given surfactant and put on ventilator soon after admission in the NICU. She was given intravenous fluids and ceftriaxone with gentamicin. Because the pulse volume was low, the child was given a normal saline bolus and dopamine infusion. On the second day, antibiotics were empirically changed to meropenem and vancomycin as the baby′s condition was deteriorating. Fresh frozen plasma (30 ml) was given twice on the second and fifth days. Blood culture in biphasic brain heart infusion medium revealed motile, Gram negative bacilli with bipolar staining [Figure - 1]A. Sub-culture on blood agar showed greyish white, smooth colonies with a slight metallic sheen and a distinctive musty odour [Figure - 1]B. MacConkey revealed non-lactose-fermenting colonies, which turned pink after 48 h [Figure - 1]C. Ashdown′s medium, a selective medium showed 3-4 mm bluish purple colonies characteristic of B. pseudomallei [Figure - 1]D. The isolate was identified as B. pseudomallei based on bipolar appearance, growth on Ashdown′s medium and characteristic biochemical reactions, including positive oxidase reaction, nitrate reduction, arginine dihydrolase activity and oxidation of glucose and lactose. Antibiotic susceptibility testing was performed by the disk diffusion test according to the Clinical Laboratory Standards Institute guidelines. [3] The isolate was susceptible to ceftazidime, cotrimoxazole and meropenem, but resistant to gentamicin, amikacin, ciprofloxacin and polymyxin B (300 µg/disc). The unusual antibiotic susceptibility pattern was also suggestive of B. pseudomallei. After three days on antibiotics, the child became afebrile. The antibiotics were continued for 10 days and the dopamine was tapered and stopped. On the 12 th day, the child was discharged. The child was active, tolerating feeds and had no respiratory distress at discharge. She was prescribed amoxicillin-clavulanate for two weeks and asked to come for follow-up. Investigations were conducted to determine the source of infection. B. pseudomallei was not recovered from the vaginal swab of the mother or environmental samples (including disinfectant solution, humidifier fluid, ventilator circuit, bed, aircondition vents, wash basin, etc.) from the NICU. Discussion Melioidosis was first reported among the morphine addicts of Rangoon, Burma (Myanmar) by Whitmore and his assistant CS Krishnaswami in 1911. In India, melioidosis was reported first in a child from Maharashtra in 1990. [4] Recently, many cases of melioidosis have been reported from India among adults, [5],[6] but there are only a few reports in children. [4],[6] Neonatal cases have been reported from the United States of America, Thailand, Malaysia and United Kingdom. [1],[7],[8],[9],[10],[11] But, to the best of our knowledge, until now, there is no report of neonatal melioidosis from the Indian subcontinent. The infection is usually transmitted by inhalation of contaminated aerosols and ingestion of or direct contact of skin lesions with contaminated water or soil. [2] Perinatal transmission and transmission through breast milk have also been observed. [9],[12] In humans, vertical transmission of this organism has been demonstrated. [10] The epidemiological characteristics of the neonatal cases of melioidosis reported from various parts of the world are summarized in [Table - 1]. In our case, B. pseudomallei was not recovered from the genital tract of the mother or the environmental samples. Hence, transmission during birth or from the environment appears unlikely. The neonate might still have acquired the infection from an unidentified environmental source either by inhalation or by direct contact of minor skin lesions with the infective source. The neonate′s mother is an agricultural labourer (rice farmer) and so she could have contracted infection through her daily contact with the soil and water of paddy fields, in which B. pseudomallei exists as a saprophyte. In the only documented case of mother-to-child transmission of neonatal melioidosis, B. pseudomallei was transmitted from an asymptomatic mother (afebrile and blood culture negative) to the neonate, but B. pseudomallei was later recovered from the post-partum cervical specimen of the mother. In our case, B. pseudomallei was not isolated from the vaginal specimen of the mother but the presence of asymptomatic bacteremia due to B. pseudomallei was not excluded as blood culture of the mother was not performed. Transplacental spread of B. pseudomallei has been demonstrated in goats although it is yet to be documented in humans. [13] Because the presence of B. pseudomallei in the mother′s blood was not excluded in our case, there is still a rare possibility of transplacental transmission from a sub-clinical infection in the mother. Although B. pseudomallei typically has a wrinkled appearance in culture medium, it is also known to produce smooth colonies. [2],[14] Lack of awareness of this variation in the colony morphology may result in misidentification of this pathogen. Based on the colony morphology in Ashdown′s agar after four days of incubation at 37°C, seven morphotypes have been described (denoted I-VII), types III and VI being smooth. [14] Our isolate resembles type III based on the size (>2 mm), smooth surface and variable colour (pale purple to dark purple). The type III strains are more efficient than type I in interacting with the macrophages and have a higher replication fitness following uptake by macrophages, which was associated with a switch to type II. Type III is also favoured under harsh environmental conditions as it is associated with increased expression of flagella and, therefore, has enhanced ability to move towards more favourable conditions. [14] Ceftazidime is the treatment of choice for melioidosis and carbapenems have been shown to be highly effective for the treatment of acute severe melioidosis with fewer treatment failures than ceftazidime. [2] Children with melioidosis do not respond to ceftriaxone and gentamicin (the empirical regimen for sepsis), which underscores the need for a high index of suspicion of this condition. Even in our case, the neonate was initially deteriorating despite being treated with ceftriaxone and gentamicin and showed improvement only when meropenem was administered. Because relapse is common with melioidosis, treatment with an oral antibiotic such as amoxicillin-clavulanate should be continued for a couple of weeks and the child should be followed-up to ensure remission. [2] The combination of chloramphenicol, doxycycline and cotrimoxazole can also be used for maintenance therapy instead of amoxicillin-clavulanate, as the latter is associated with a relapse rate of 16% compared with 4% with the former regimen. [15] But, in children, amoxicillin-clavulanate is preferred because of its lower toxicity. [2] Our report of neonatal melioidosis alerts the paediatricians and microbiologists to the possibility of this infection even among neonates, emphasizing the need to speciate non-fermentative Gram negative bacteria, especially when recovered from sterile sites, which may otherwise be ignored as contaminants. A better understanding of the morphological appearance, cultural characteristics and biochemical reactions of B. pseudomallei and its potential to cause infection in neonates will aid in increased recognition of neonatal melioidosis. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09075f1.jpg] [mb09075t1.jpg] |
| |||||||||

{kind=link}
{kind=link}