 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
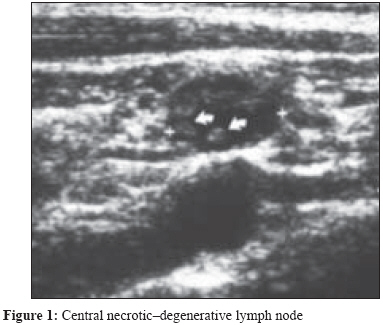
Indian Journal of Medical Microbiology, Vol. 27, No. 3, July-September, 2009, pp. 272-275 Case Report Familial tularaemia Peker E, Ayaydin A, Duran N Department of Pediatrics, Medical Faculty, Mustafa Kemal University, Hatay Date of Submission: 21-Dec-2008 Code Number: mb09079 PMID: 19584516 Abstract Tularaemia is a zoonotic disease caused by Francisella tularensis . In this report, we have presented an early stage case of tularemia with fever and pharyngitis and two cases from the same non-endemic region with typical lymphadenitis. All three patients were treated with non-specific medications in healthcare centres, the treatment being directed towards symptoms resembling those of upper respiratory tract infections. However, there was no regression in their complaints. Because the first case had been treated earlier, his lymphadenopaties regressed and there was no suppuration. The other two cases, which had been suspected to be exposed to the same pathogen based on their histories, were at a mild acute phase and presented to our clinic with typical lymphadenitis. The diagnoses of each of the three patients were made serologically. An early clinical recovery was achieved in the first patient with streptomycin (1 x 1 g/day im) and doxycyline (2 x 100 mg/day peroral) therapy. The therapy was prolonged to 4 weeks in the other two cases according to lymph node response and no complications occurring in their follow-ups. It can be concluded that tularaemia should be considered in the differential diagnosis of patients with fever, pharyngitis, conjunctivitis and cervical lymphadenopathies that do not respond to β -lactam antibiotics.Keywords: Children, Francisella tularensis, treatment, tularaemia Tularaemia is a zoonotic disease caused by Francisella tularensis , [1],[4] a small, fastidious, non-spore-forming, aerobic gram-negative coccobacillus. It is non-motile, non-piliated, and has a thin capsule composed mostly of lipid. [2] This bacterium was first identified in 1912 following reports of a plague-like illness in ground squirrels in Tulare County, CA. Since the discovery of this pathogen, four sub-species have been identified that exhibit distinct virulence and biochemical profiles as well as characteristic geographic distributions. Human disease is primarily associated with two F. tularensis sub-species: the highly virulent F. tularensis subsp. tularensis (type A), which is found only in North America, and the moderately virulent F. tularensis subsp. holarctica (type B), which is endemic throughout the Northern Hemisphere. Serovar B is less virulent, often results in subclinical infection, and has a worldwide distribution in the Northern hemisphere between latitudes 30 and 71 degrees north, including the continents of Europe, Asia, and North America. [3] Tularaemia outbreaks have previously been reported in various geographical locations in Turkey. In this report, we report three cases from the same family that lived in the city of Bitlis in Turkey. This is first report from this non-endemic region. Case Reports Case 1 Case 2 Case 3 Discussion The clinical picture of tularaemia may vary depending on several factors, such as the route of transmission, virulence of the microorganism strain, and the immune condition of the host. [1],[4] F. tularensis may enter the host through cuts or abrasions in the skin, by penetration through the mucous membranes of the eye, respiratory tract or oropharynx, or by percutaneous inoculation by arthropods. [5],[6] However, the most important source of F . tularensis transmission is the water supply because these bacteria may remain alive in water for several months. In our opinion, the water was contaminated with infected rodents. Because the patients had mentioned that they had played around the lake and also swam in that lake, we considered that the lake water had caused the disease and our hypothesis was supported by other patients who had not presented to the other departments of the hospital with similar symptoms. There is a probability that a ship may have sunk in that lake and, therefore, the children could have been infected. The reason for this consideration was that there were no patients who somehow had a connection with the lake water in the following days. All our three cases were accepted as having oropharengeal tularaemia. Most tularaemia infections are acquired from contaminated water or food. There is direct invasion of the oropharynx by bacteria in the oropharengeal form. In these cases, the most important complaints were sore throat and fever. For this reason, it was confused with angina. Because of this confusion, non-specific antibiotic therapy had been administered to these patients. Clinical manifestations appear after an incubation period of 2-10 days. The most common clinical syndromes are ulceroglandular and glandular tularaemia, which account for 80% of the reported cases. Recent cases have shown that the oropharyngeal type is more prevalent in our country. [1],[5] All these three cases were accepted as oropharengeal tularaemia, and this is the first report from Bitlis in the east of Turkey. The bacterial culture of F . tularensis culture is not performed routinely in clinical laboratories. The laboratory diagnosis of tularaemia is usually confirmed by a serum agglutination test using commercially available antigens. [7],[8] Thus, we used agglutination tests. However, as such in our patients, non-specific cross-reactions can occur in patients with brucella antibody. The diagnosis of brucella was excluded using the brucella tube agglutination test, which was negative. The cases were defined according to Centers for Disease Control and prevention (CDC) guidelines. [9] The result of the sample blood of the first patient had turned out to be negative. The serum samples could be obtained from the patient during the early stages of infection. We think that this played a big role in explaining why the first sample was seronegative. Streptomycin is accepted to be the drug of choice in tularaemia, but it is usually combined with the antibiotic doxycycline or chloramphenicol. F . tularensis is resistant to all β -lactam antibiotics. [10] In the presented cases, the therapy of streptomycin (1 x 1 g/day im) combined with doxycycline (2 x 100 mg/day peroral) was given to all the patients according to the susceptibility data of Turkish isolates. [11] It was determined that combined antibiotic therapy was effective and the therapy was prolonged to 4 weeks. Antibodies are generally detectable at the end of the second or during the third week of illness. Thus, empirical antibiotic therapy must be initiated before serological confirmation of infection. The differential diagnoses include tuberculosis, sporotricosis, primary syphilis, pharyngitis of streptococcosis, infectious mononucleosis, adenoviral infections, cat scratch disease, and acute toxoplasmosis. [1],[9],[10] These diagnoses can be excluded from the history of the patient, laboratory findings, and the symptoms on the physical examination. It can be concluded that tularaemia should be considered in the differential diagnosis of patients with fever, pharyngitis, conjunctivitis, and cervical lymphadenopathies. Furthermore, early diagnosis and treatment of tularaemia are important to prevent abscess formation, and patients with delayed diagnosis may benefit from prolonged therapy. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09079f1.jpg] [mb09079f2.jpg] |
| |||||||||
{kind=link}
{kind=link}