 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 289-300 Review Article Established and potential risk factors for Clostridum difficile infection *C Vaishnavi Department of Gastroenterology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India Correspondence Address: Department of Gastroenterology, Postgraduate Institute of Medical Education and Research, Chandigarh - 160 012, India, cvaishnavi@rediffmail.com Date of Submission: 27-May-2009 Code Number: mb09087 PMID: 19736396 DOI: 10.4103/0255-0857.55436 Abstract Clostridium difficile is the aetiological agent for almost all cases of pseudo membranous colitis and 15-25% of antibiotic associated diarrhoea. In recent years, C. difficile associated disease (CDAD) has been increasing in frequency and severity due to the emergence of virulent strains. Severe cases of toxic mega colon may be associated with mortality rates of 24-38%. The prevalence of CDAD is global and the incidence varies considerably from place to place. In the initial stages of its discovery, C. difficile infection was regarded mainly as an outcome of antibiotic intake and not as a life threatening disease. Intervention by man has produced conditions making C. difficile a significant cause of morbidity and mortality. The recent outbreak of CDAD in Quebec has sent the alarm bells ringing. Apart from a threefold increase in the incidence of CDAD, clinicians have also reported a higher number of cases involving toxic mega colon, colectomy or death. Among all the risk factors, inclusive of the host and the environmental factors, antibiotics are the most important ones. Surgical patients comprise 55-75% of all patients with CDAD due to the fact that perioperative prophylaxis requires the use of antibiotics. However, other drugs such as immunosuppressants and proton pump inhibitors are also important risk factors. Thus CDAD is a growing nosocomial and public health challenge. Additionally, the recognition of community acquired CDAD signals the presence of several risk factors. In this review, the established and potential risk factors of CDAD, along with the epidemiology, diagnostic modalities, management and preventive measures of the disease have been elaborated.Keywords: Antibiotic associated diarrhoea, C. difficile, risk factors. diagnosis, prevention Introduction Clostridium difficile is a spore-forming, anaerobic, Gram-positive bacillus responsible for nosocomial diarrhoea in economically developed countries. It is also the aetiological agent for almost all cases of pseudo membranous colitis (PMC) and 15-25% of antibiotic associated diarrhoea. [1],[2] In recent years, C. difficile associated disease (CDAD) has been reported to be increasing in frequency and severity due to the emergence of virulent strains. Acute cases of CDAD can lead to enteric ulceration or bleeding. Clinical symptoms commonly seen include diarrhoea, fever, increased faecal leukocytes, abdominal cramping and dehydration. Potentially significant complications responsible for morbidity and mortality include hypoalbuminaemia, toxic mega colon, colonic perforation and PMC. According to Poutanen and Simor [3] severe cases of toxic mega colon may be associated with mortality rates of 24-38%. C. difficile , originally recovered as a component of the faecal flora of healthy newborn infants is now known to be present in the stool of up to 50% healthy neonates. It can also be isolated from the stool of five per cent healthy adults, usually in low numbers. Thus it appears that C. difficile is normally a harmless environmental organism which becomes an opportunistic pathogen when circumstances permit. As a matter of fact, intervention by man has produced conditions making C. difficile a significant cause of morbidity and mortality. Toxigenic C. difficile strains produce two highly potent exotoxins - toxins A and B that share 63% of amino acid homology and are recognised as the main virulence factors. Even though C. difficile strains generally produce both the toxins, A - B + types are also increasingly being reported. Another toxin identified (iota-like toxin) is a binary toxin, the role of which in the pathogenesis of CDAD is unclear. Majority of the strains harbouring the binary-toxin genes are also A + B + . Up to two per cent of C. difficile are estimated to produce only binary toxin and 4-12% of isolates are positive for this toxin. Thus, toxigenic strains will possess one or more of any of these three toxins. Non-toxigenic isolates are not responsible for diarrhoea as they do not produce toxins. However, patients can harbour both toxigenic as well as non-toxigenic strains at any given point of time. In spite of having high numbers of the organism in their colons, the toxin in their stools could vary from minimal to a large amount. The first event in the occurrence of CDAD involves alteration of the indigenous colonic micro flora, followed by C. difficile colonisation when the individual is exposed to the organism or its spores. Diarrhoea and colitis are caused by the release of toxins having potent enterotoxic and cytotoxic properties. Two-thirds of healthy adults have serum immunoglobulin G and intestinal secretory IgA antibodies to toxin A. These antibodies may inhibit in vitro toxin A binding to its specific intestinal receptor. Kyne et al, [4] reported an association between defective humoural response to toxin A and a more severe form of C. difficile infection. Acute inflammatory infiltration occurs in the colonic mucosa due to the destruction of epithelial cells with increased permeability of the tight junctions. This leads to fluid secretion, inflammation and mucosal damage leading to diarrhoea or PMC. Katyal et al, [5] reported a significant disturbance in the intestinal brush border enzymes in patients with C. difficile diarrhoea. The organism is known to infect up to 20% of individuals admitted to hospital and who are on antibiotic treatment. After a first recurrence, risk of another infection increases up to 60%. On an annual rate C. difficile causes approximately three million cases of nosocomial diarrhoea in the United States alone with the annual cost of treatment being greater than $1.1 billion [6]. Thus, CDAD is a growing nosocomial and public health challenge. In addition to this, community acquired CDAD signals the presence of several risk factors other than antibiotics. Early identification of patients with high risk of CDAD may help in the clinical management of the disease. In this review, the established and potential risk factors of CDAD, along with the epidemiology, diagnostic modalities, management and preventive measures of the disease have been elaborated. Epidemiology C. difficile infection is a serious condition with mortality up to 25% in frail elderly patients. However, age is a non-specific predictor of severe CDAD. The younger age group was not considered to be at risk previously. However, Healthcare Commission from England has reported that 20% CDAD patients belong to the younger age group and the disease increased 50-fold in an eight-year period from 1990 to 2007. [7] It is speculated that immunosuppression could be the factor responsible for affecting the younger age group. Children under the age of two years are generally carriers and clinical disease is rarely seen among them. Only a few reports of histopathologically and endoscopically proven cases of PMC in children have been recorded. Children with fatal diseases usually have underlying Hirschsprung's disease or a haematological malignancy. It is believed that the toxins are unable to attach to the mucosa of newborns or that infants are protected from toxins by maternally acquired antibodies. It has also been postulated that specific dietary substrates may be required for full expression of toxins or that the host mucous could also play an important role by interacting with toxin or masking receptors. Up to 50% of infants acquire toxigenic C. difficile in the hospital nursery. In some cases, asymptomatic infants can have levels of toxin comparable to those seen in adult patients with PMC. On rare occasions, C. difficile disease may occur in compromised infants treated with antibiotics. The prevalence of C . difficile -associated colitis is global and the incidence varies considerably from place to place. In developing countries like India, C. difficile infects 15-30% of paediatric and adult patients taking antibiotics. [8],[9],[10],[11],[12],[13] Studies on C. difficile -associated diarrhoea are limited, probably due to the lack of technology and facilities for culturing anaerobic pathogens. C. difficile has been isolated from the faeces of adults and children in Polish hospitals, where it is a significant aetiologic agent of hospital-acquired diarrhoea. [14] Despite the fact that toxigenic C. difficile was isolated from only 1.8% of the patients analyzed, the increase in widespread and indiscriminate use of antibiotics in Eastern Europe raises the concern of CDAD becoming a significant cause of hospital-acquired diarrhoea in Eastern Europe. [14] Shehabi et al. [15] demonstrated that C. difficile is a common pathogen recovered from hospitalised patients in Jordan with symptomatic diarrhoeal illness or without diarrhoea as a result of antimicrobial usage or due to cancer chemotherapy. Thus C. difficile has emerged as the most common cause of hospital acquired diarrhoea due to broad-spectrum antimicrobial use. Even though antibiotics are regarded as the primary risk factor, additional host-related and environmental factors control the severity of the disease. Clostridium difficile- induced enteric disease is common place in both nursing homes and hospitals. It is quite obvious that C. difficile PMC may result from nosocomial infections as case clusters occur in hospital settings with the hospital care workers and attendants of patients becoming carriers of the organisms. The percentage of patients who become carriers may be higher than the number of patients who develop serious diarrhoea and colitis following infection. The incidence of C. difficile has greatly increased in recent years. The overall incidence of CDAD in Oregon was 3.5 case patients per 10,000 residents in 2002 and the incidence increased from 1.4 to 3.3 cases per 1000 hospital discharges from 1995 to 2002. [16] The average mortality associated with CDAD is around 17% but in the older adult population it is much higher because of age-related changes and the presence of multiple co-morbidities. In the initial stages of its discovery, C. difficile infection was regarded as an outcome of antibiotic intake and not as a life threatening disease. However, the recent outbreak of CDAD in Quebec [17] has sent the alarm bells ringing. Apart from a three-fold increase in the incidence of CDAD, clinicians have also reported a higher number of cases involving toxic mega colon, colectomy or death. Mortality within 30 days increased from 4.7 to 13.8% in a span of about a decade. [18] Earlier epidemics of C. difficile involved single institutions. At least 12 hospitals in the entire Estrie region saw record numbers of CDAD cases in the Quebec epidemic. The strain involved in 82% cases and resistant to some fluoroquinolones was typed as NAP1/BI/027 (North American PFGE type I/ restriction endonuclease analysis BI/ribotype 027). [19] This strain was found to produce greater than 16 times toxin A and 23 times toxin B in addition to the binary toxin. [20] This global epidemic strain has also been reported to cause outbreaks in parts of continental Europe. [1] McDonald et al, [19] found NAP1/BI/027 strain in eight institutions, in six different states in the United States and it represented more than 50% of the isolates from five institutions. This strain has also been reported from Great Britain, The Netherlands and Belgium. [22] C. difficile is also being reported more frequently even from non hospital-based settings, such as community-acquired cases. C. difficile infects a wide variety of domestic as well as wild animals, and the same ribotypes as those found in animals and their meat products was found to be associated with human infection suggesting community acquisition of the infection. CDAD Risk Factors The human intestinal tract harbours a complex community of normal flora that constitutes an extremely important defence mechanism against the establishment of enteric pathogens. Disturbances in the ecosystem by human intervention can lead to the establishment of pathogenic organisms. C. difficile is one such pathogen that can thrive and produce toxins and result in clinical manifestations of CDAD. There are several established and potential risk factors for CDAD; the most important among them are elaborated as follows: Drugs Among all the risk factors involved, antibiotics are the most important risk factor. Other drugs such as immunosuppressive agents, proton pump inhibitors and cancer therapeutics are also significant risk factors for CDAD precipitation. Each class of drug has been separately dealt with. (i) Antibiotics: CDAD became prevalent in the 1960s and 1970s with the introduction of broad-spectrum antibiotics to clinical practice. Disruption of normal intestinal flora by antibiotics is a well-known risk factor for CDAD. [11],[12] Clindamycin was the first antibiotic implicated in CDAD. Now it is well known that penicillin, ampicillin, cephalosporin and fluoroquinolones can all precipitate CDAD. All antibiotics including vancomycin and metronidazole, commonly used to treat CDAD, have been found to be risk factors for subsequent CDAD. Risk is greater when the patients are on multiple antibiotics and undergo longer course of therapy. It is incorrect to use the term 'antibiotics' in isolation as almost any antimicrobial agent including antifungal and antiviral can induce the disease. More than 90% of health care associated CDAD occur during or after treatment with antimicrobials. Earlier work demonstrated the prominent role of clindamycin as a risk factor for CDAD. Studies carried out after 1980 showed that cephalosporin is also the most common agent implicated in nosocomially acquired CDAD. In outpatient settings, antibiotics such as ampicillin, amoxicillin or amoxicillin-clavulanate combination are also important and common causes. Less commonly implicated antibiotics are macrolides, tetracyclines, sulphonamides, trimethoprim, chloramphenicol and penicillin other than ampicillin/amoxicillin. A substantial overlap of antibiotic use with consequent colonisation by C. difficile results in C . difficile -induced diarrhoea. Any particular antibiotic can be specifically associated with CDAD based on its frequency of use, route of administration and effect on the colonic micro flora. Recent history of fluoroquinolone administration is an important risk factor for CDAD. [17] Even though C. difficile is sensitive to vancomycin and metronidazole, there is an increasing emergence of strains with reduced susceptibility to these two antibiotics. Vaishnavi et al , [10] report 30% positivity for C. difficile toxin in hospitalised patients of all age group receiving single to multiple antibiotics for various ailments, but only in seven per cent of samples from patients not receiving antibiotics. When only adult population were investigated, the positivity for C. difficile toxin was 19.4% in the antibiotic receiving hospitalised patients. [11] Many hospitalised adults become asymptomatic carriers after receiving antibiotics. The case mix on wards and bays within wards is important because of a potential herd immunity effect. That is, if only a few patients in a ward have been exposed to antibiotics, most of those who have not been treated with antibiotics will retain their normal colonic bacterial flora and will not develop C. difficile associated diarrhoea. The potential for an outbreak depends on increased use of antibiotics as well as increased number of elderly people. During the last decade health workers at a Pittsburgh tertiary care hospital reported increased incidence of nosocomial CDAD with marked increase in severity of cases requiring colectomy or ending in death. This was attributed to increased use of fluoroquinolones particularly levofloxacin, though clindamycin and ceftriazone were also identified as risk factors. In the Quebec epidemic, 8000 CDAD cases were reported in a one-year period and fluoroquinolones were the most important risk factor. [17] Loo et al, [18] in a prospective case controlled study in 12 hospitals in Quebec with 1703 CDAD patients showed a higher mortality, with cephalosporins and fluoroquinolones as risk factors. The NAP1/027 strain detected globally is also found to be resistant to fluoroquinolone antibiotic and poses a great risk. Severe cases of CDAD with this epidemic strain were detected in Germany for the first time, in 2007, and were strongly associated with receipt of antibiotics, particularly cephalosporins and fluoroquinolones in the three months before the onset of symptoms. [23] Saxton et al [24]. using a 3 stage chemostat gut model showed that fluoroquinolones such as ciprofloaxacin, levofloxacin and moxifloxacin all have propensity to induce C. difficile infection. (ii) Immunosuppressive Agents: Infection is the leading cause of morbidity and mortality in the early post-transplant period in patients taking immunosuppressive agents. Immunosuppressive drugs have been reported to be associated with the development of CDAD. [25],[26] Faulty immune response to C. difficile toxins has been quoted as one of the major host factors predisposing patients to the development of symptomatic CDAD. [1],[27] Patients at highest risk for fulminant disease include those who have recently received immunosuppressive therapy or have undergone surgical procedures and those with a history of CDAD. [27] The ability of the immune system of the host to produce protective antibodies against C. difficile toxins plays an important role in reducing the severity of disease and preventing further recurrences. The host antibody response is a major determinant of the disease outcome. Serum levels of IgG antibody against toxin A are found to be higher in patients with a mild CDAD than in those with prolonged or severe diarrhoea. Patients with C. difficile colonisation and a serum IgG response to C. difficile enterotoxin usually become asymptomatic carriers while patients lacking protective immunity develop diarrhoea and colitis. [4] Even if the immune response to C. difficile toxins is inadequate, it will predispose patients to severe, prolonged and recurrent C. difficile diarrhoea. [4] Patients receiving immunosuppressive drugs are debilitated and therefore are unable to mount an effective IgG antibody response against C. difficile toxin A thereby increasing the risk for CDAD. [4] Though the ability to mount an immune response is not protective against C. difficile colonisation, it is associated with decreased morbidity, mortality, and recurrence of C. difficile -associated diarrhoea. [4] C. difficile colitis may occur without prior use of antibiotics in immunosuppressed patients. Exposure to corticosteroids is significantly associated with an increased risk of CDAD relapse warranting a longer treatment course. C. difficile colonisation is more frequent in intensive care and oncology units where broad spectrum antibiotics and immunosuppression are wide spread. West et al, [25] investigated to find whether immunosuppressed transplant recipients were more prone to CDAD and its complications and observed an increased incidence of C. difficile colitis in paediatric kidney-pancreas recipients. They reported overall eight per cent incidence of CDAD with 16% in the paediatric kidney group and 15.5% in the kidney-pancreas group. Keven et al, [26] reported that 5.5% of patients after solid organ transplantation developed C. difficile colitis at a median of 30 days after transplantation. Dallal et al. [27] reported 31% incidence of CDAD in lung transplant patients compared to 1.6% overall. Wong et al, [28] also reported that C. difficile and medication were the commonest colorectal cause of morbidity after orthotopic liver transplantation in addition to ulcerative colitis and cytomegalovirus infection. Administration of tacrolimus, an immunosuppressive agent indicated for prophylaxis of organ rejection after allogeneic kidney or liver transplant, resulted in the development of CDAD. [29] Ulcerative colitis patients unresponsive to corticosteroids may require long time immunosuppressive treatment which may result in multiple infections, inclusive of C. difficile. [30] Diarrhoea is a common manifestation after liver transplantation and a side effect of immunosuppressive medication with C. difficile as one of the aetiologic agents. The frequent use of antibiotics, suppression of antibody-mediated response to toxins, and longer and more frequent hospital admissions can be attributed to increased susceptibility to CDAD among solid organ transplant patients. [25],[26] The incidence density of CDAD was higher and the disease more often typical and/or complicated in cystic fibrosis patients who had undergone lung transplantation compared to non-transplanted patients. [31] Five leukaemic patients treated with immunosuppressive, died from secondary complications of PMC [32]. The use of immunosuppressives may account for a large number of CDAD patients without prior use of antibiotics. As the use of immunosuppressive increases, the incidence of CDAD will also rise further. (iii) Proton Pump Inhibitors: Colonisation of normally sterile upper gastrointestinal tract can be a consequence of gastric acid suppressive use due to raised pH of stomach resulting in increased risk of enteric infections including CDAD. Gastric acid secretion acts as a barrier for enteric pathogens. Proton pump inhibitors (PPI) inhibit the gastric acid secretion by interfering with the activity of H + /K + -ATPase of the parietal cells and may thus contribute to the pathogenesis of CDAD by altering the intestinal flora. The total volume of prescribing for PPI increased 10-fold in the United Kingdom between 1992 and 1995 [33]. In the United States, expenditure on PPI for a single year exceeded $12 billion, making it one of the widely prescribed drug classes in sales. [34] The risk of CDAD due to PPI would have major public health implications. Patients are about twice as likely to develop CDAD with PPI, due to increased survival of spores. Studies from hospitals and community have examined the association between PPI use and the risk of CDAD with contradictory results. PPI use was a significant risk factor for CDAD in a retrospective case control study. [35] Clinical studies carried out on inpatients at Montreal teaching hospitals comparing the risk for development of CDAD in those who received gastric acid suppressive therapy and those who did not revealed that PPI use was associated with an elevated risk of development of CDAD. However, Pepin et al, [17] reported that elevated risk of CDAD with PPI occurred in univariate analysis but not after adjustment for co-morbidities on multivariate analysis. Al-Tureshi et al, [36] have reported that low albumin level, a recent admission to a nursing facility, and the use of PPI are the important risk factors for CDAD while assessing institutional patients with diarrhoea. Another study found CDAD to be independently associated with antibiotic use and acid suppression therapy. [37] Kaur et al, [38] found that BALB/c mice treated with PPI had a higher experimental colonisation with C. difficile, enhanced myeloperoxidase activity as well as greater level of epithelial damage, oedema and neutrophilic infiltrates in the colon as compared to control untreated animals. Cadle et al, [39] found that PPI therapy was associated with an increased risk of recurrent colitis due to C. difficile, Jayatilaka et al, [40] in a five year study period found that PPI usage correlated exactly with the overall annual increased CDAD incidence and believed that the widespread prescription of PPI could be responsible. Nachnani et al, [41] reported that PPI therapy was independent and the only risk factor associated with an increased length of hospital stay in CDAD patients. Gastric acid-suppressive drug use was also associated with an increased risk of community acquired CDAD [42] even though Lowe et al, [34] did not find an association between PPI therapy and hospitalisation for community-acquired CDAD among elderly patients treated with broad-spectrum antibiotics. Proton pump inhibitor may be a risk factor for CDAD because of (i) the survival of spores facilitated by elevated gastric pH levels and (ii) due to the effect of PPI on immune function or on the toxin production of the organism. Inhibition of gastric acid removes a defence against ingested bacteria and spores, increasing the risk of some forms of gastroenteritis. Acid suppressive agents are among the most frequently prescribed medications in most parts of the world. It is in this context that the contribution of these agents by potentially increasing the pool of susceptible hosts to the increasing rates of CDAD needs to be considered and more completely characterised. Thus the risk of CDAD in hospitalised patients receiving antibiotics may be compounded by exposure to PPI therapy. Curtailing the inappropriate use of PPI therapy may help prevent the increased hospital stay by CDAD patients and reduce overall costs of management and therapy. (iv) Cancer Therapeutics: Administration of cancer chemotherapeutic agents possessing antibacterial properties may also result in sufficient disturbance of the intestinal micro flora to allow colonisation with C. difficile . This can occur without the associated use of antibiotics. Emoto et al, [43] reported severe CDAD in 6.1% of patients receiving cisplatin based combination chemotherapy for ovarian malignancies. Resnik and Lefevre [44] described development of fulminant C. difficile colitis in a 66 year old patient with ovarian cancer who received paclitaxel and carboplatin chemotherapy. It is likely that Crohn's disease patients with mildly active disease treated by mesalamine may also end up with CDAD. Kumar et al, [45] reported that 19 out of 58 patients treated with methotrexate or mesalamine for psoriasis were positive for C. difficile toxins. Thus the combination of the environmental presence of C. difficile in health care settings and the number of people receiving antibiotics, immunosuppressives, proton pump inhibitor or cancer therapeutics in these settings can result in frequent outbreaks. Non Drug Risk Factors Apart from the use of drugs several other factors can determine whether or not a patient develops a C. difficile infection. The list of such factors is exhaustive and many a times several factors may be interlinked. Briefly they include: (i) Host risk factors Age: The incidence of C. difficile infection rises with increasing age, particularly so in the elderly. This is partly because of increased use of antibiotics in older patients and also due to the presence of predisposing factors such as severe underlying illness.
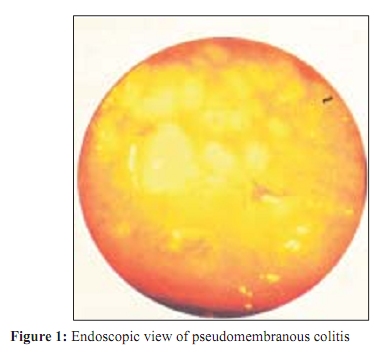
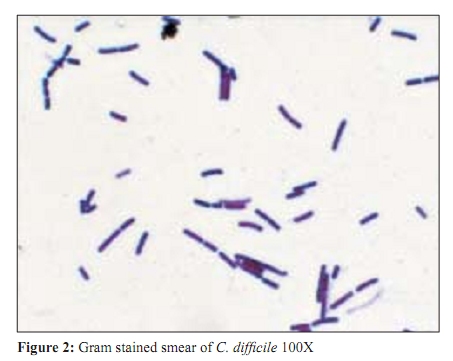
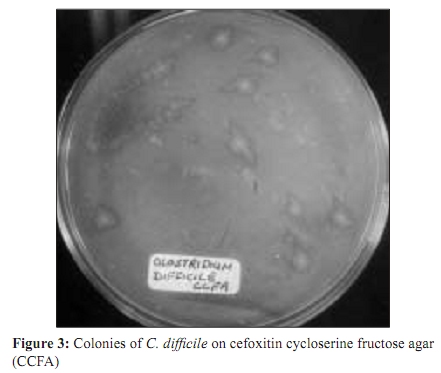
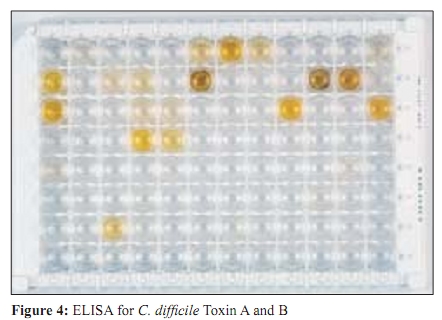
(ii) Factors Associated with the Pathogen Even though C. difficile is present in up to five per cent of healthy adults and 50% infants and children, it is not a significant component of gut micro flora. However, large population of C. difficile organisms can be established in antibiotic treated hosts, acquiring a complete flora. Thus precipitation of CDAD also depends on (a) the size of C. difficile population (b) adhesive capability of the C. difficile strain to the intestinal receptors (c) production of the requisite cytotoxins by the C. difficile strain and (d) the presence of other organisms that affect toxin expression or activity particularly by limiting the available nutrients. (iii) Environmental Risk Factors Hospitals, nursing homes, childcare facilities, intensive care and high dependence units are major reservoirs for C. difficile . Hands of health care workers, environmental contamination through commodes, bathtubs, thermometers, stethoscopes, etc carry great risk of cross infection. Environments around patients are more contaminated than those around the carriers. The speed of diagnosis of CDAD can be very useful in prompting immediate treatment as well as in controlling the environmental spread of infection to other patients. Cross infection due to cleaning material such as beds, clinical waste, etc. during patient changeover requires good infection control practices to prevent faecal soiling. CDAD patients who have become asymptomatic are not considered as risk to others even if they excrete toxigenic C . difficile , provided they follow good personal hygiene particularly after defaecation. Dumsford et al, [48] reported that in the context of CDAD outbreak, environmental contamination was common in non-isolation rooms, physician and nurse work areas and on portable equipments. Environmental contamination around asymptomatic carriers than noncarriers reflects poor toilet capacity and environmental cleaning. Patients should be looked after in a clean environment and should be educated to maintain personal hygiene. The rate of colonisation among community residents is one to three per cent in contrast to about 20% among adult hospitalised patients. Even community dwellers not exposed to antibiotics may experience sporadic outbreaks of CDAD. Diagnostic Modalities Clostridium difficile associated diseases can be suspected and/or diagnosed clinically, endoscopically, radiologically as well as by identification of aetiological agent and by toxin assays. Clinical The clinical presentations in increasing order of severity, include asymptomatic carriage, antibiotic associated colitis without pseudomembrane formation, PMC and fulminant colitis with catastrophic transmural inflammation and myonecrosis. The most severe forms though are the least common. Various signs and symptoms help to diagnose the disease clinically. Profuse watery, green, foul smelling or bloody diarrhoea along with abdominal cramps is the hallmark of PMC. Peripheral blood polymorphonuclear leucocytosis and increased number of faecal leucocytes are other important features. When benign diarrhoea occurs with antibiotic use, no leucocytosis is seen. Patients may experience occult colonic bleeding, and rarely may develop frank haematochezia. High fever occurs with temperature ranging from 38-39°C. However, fever as high as 41°C has been recorded. Other common systemic manifestations include nausea, anorexia, malaise, dehydration and delirium. When PMC presents without accompanying diarrhoea, the delay in diagnosis could be lethal with development of toxic mega colon or perforation. Endoscopy Pseudomembranous colitis can be detected as multiple yellow-white friable plaques, a few centimetres in size attached to the underlying mucosa [Figure - 1]. The major advantage of endoscopy is that diagnosis of PMC can be done both quickly and accurately, which help to avert emergency abdominal surgery. However, 10% cases of PMC go undetected when only sigmoidoscopy is done without colonoscopy as PMC is more likely to occur in the proximal colon first. Moreover, PMC is a late manifestation of the disease and is not likely to be present always. Mild cases are often described as non-specific colitis. Biopsy and sigmoidoscopy have limited use because of the patchy nature of the distribution of the membrane. Oedema, blurring of the vascular pattern and thickening and blunting of the haustral folds are also present. When PMC has been established, biopsy is confirmatory, but not essential. However, when PMC has not been detected, biopsy is desirable if the mucosa appears inflamed, friable, granular or haemorrhagic, to reveal histologic changes typical of PMC. Endoscopy should be avoided in patients with paralytic ileus or colonic dilatation because of the risk of perforation. The disadvantages of endoscopy are the high cost of the procedure and extensive colon preparation. It is better reserved for special situations, such as when the patient is seriously ill and the results of rapid but not highly sensitive non-invasive tests are negative or delayed and C. difficile diarrhoea is strongly suspected. However, it should be noted that other disorders may also produce pseudomembranes, for example a cytomegalovirus infection. Si-Wook et al [49] reported 6 cases of PMC with diarrhoea after administration of rifampicin as a treatment for active pulmonary tuberculosis. Radiology Pseudomembranous colitis can be sometimes diagnosed by computed tomographic (CT) scan when diarrhoea is absent but abdominal pain, fever and leucocytosis occur. It reveals diffusely thickened or oedematous colonic wall with pericolonic inflammation. CT scan findings are not pathognomonic of PMC, but it prompts strong consideration for initiation of specific therapy. In a recent study, Pudhota et al [50] described a case of an 80-year-old male with multiple co-morbidities and history of recent antibiotic treatment for chronic obstructive pulmonary disease and exacerbation presented with fever, shortness of breath and abdominal pain, but no diarrhoea. Transverse colon appeared to be markedly dilated in an abdominal X ray and thickened loops in CT scan, which was later, found to be due to C. difficile infection. Thus an unusual combination of toxic mega colon without antecedent diarrhoea should be recognised as an atypical manifestation of C. difficile PMC. Identification of Aetiological Agent Clostridium difficile is a Gram positive bacillus with terminal elongated spores slightly wider than the bacillary body cells measuring 6-8 µm in length and 0.5 µm in width [Figure - 2]. It readily grows on selective media such as cefoxitin, cycloserine, fructose agar (CCFA) with or without alcohol shock. It is uniformly Gram positive in young cultures, but may become Gram negative after 24-48 h. C. difficile is a strict anaerobe. Colonies are 2-3 mm in diameter, irregularly circular, flat to slightly raised, semi-translucent and white with a glossy but rough and often pitted surface [Figure - 3]. White colonies are characteristically associated with sporulation. The characteristic odour of the colonies is that of horse / elephant's manure which is also an important identification aid. Colonies of C. difficile usually show a yellow-green or chartreuse fluorescence when exposed to long wave ultraviolet light on blood agar after incubation for 48 h. Organism is non-haemolytic on horse blood agar and produces neither lipase nor lecithinase on egg yolk agar. Glucose is fermented but not maltose, lactose or sucrose. Indole and hydrogen sulphide are not produced and nitrate is not reduced. Use of cefoxitin cycloserine fructose broth supplemented with 1% Sodium taurocholate for enrichment of C. difficile enhances its recovery. The advantage of culture is that it is a low cost sensitive and a good method. However, the disadvantages are multifold. The efficiency of culture varies from laboratory to laboratory. It also depends upon the presence of spores or viable vegetative cells. Biochemically, the procedure of identification through culture is thus cumbersome and requires several days for results. Moreover it would require a follow-up toxin testing as only about a third of the colonised isolates produce toxin. It is a technically challenging job and unattractive as a screening test. The advantage of the culturing method is that the organism is available for epidemiological and antibiogram typing which may be beneficial when outbreaks occur. Toxin Assays Various methods are available to detect toxins in the faecal samples. (i) Tissue culture: Tissue culture has been regarded as the gold standard in laboratory diagnosis of C. difficile toxin. It detects toxin B and is highly specific. It can detect as little as 1.0 pg of toxin B making it the most sensitive test available. Toxin identification is confirmed with C. difficile antitoxin or antitoxin against C. sordellii , which produces the cross-reacting toxins known as lethal toxin and haemorrhagic toxin. However, it is the least controlled test and non-specific reactions are common in laboratories. The addition of too much faecal material to the tissue culture well can cause false positive reactions. A final dilution of 1:40 to 1:50 is recommended by commercial tests. Specimens may also cause nonspecific cell rounding that is neutralised not only by the specific antitoxin but also by neutral serum. Cell lines that may be used include Vero, Hep 2, Chinese hamster ovary, HeLa cells and MRC-5 lung fibroblasts. However, many disadvantages accompany tissue culture technique. The maintenance of cell cultures is very difficult. The procedure is cumbersome, expensive and time consuming. It requires a well-developed infrastructure and cannot be done in ordinary laboratories. Moreover, the procedure requires a turn-around time of 48-72 hours. Sometimes a non-specific cytopathic effect can also occur in about 2% of the cases due to a viral agent or another bacterial enterotoxin such as that of C. perfringens , rendering any interpretation difficult. False negatives have also been encountered in stored samples because of degradation of toxins by toxin degrading enzymes like proteases or by delay in transportation or by medication, as some cell lines are less sensitive than others to the cytopathic effect of the toxin. In fact, a negative cytotoxicity assay does not completely rule out C. difficile as the cause of diarrhoea as 30% of patients may be missed. (ii) Counter immunoelectrophoresis: Detection of toxin by means of counter immunoelectrophoresis lacks the required levels of sensitivity and specificity for satisfactory diagnostic test. Moreover, the procedure is expensive and cumbersome. (iii) Dot immunobinding assay: The test is like any other enzyme immunoassay except for the fact that it is carried out on the surface of individual membrane cassette. Stool supernatant is made to pass through a filter onto the membrane and then made to react to mouse monoclonal antibody to C. difficile toxin. Appropriate enzyme conjugate and substrate are added to visualize the blue coloured dot. However the presence of excessive amount of debris can cause difficulty in interpretation of the results. Moreover, the reagents used are again expensive and unaffordable for routine use. (iv) Enzyme immunoassays: Several commercial kits available are designed to detect either toxin A alone or both toxins A and B in stool specimens [Figure - 4]. The advantage of using enzyme-linked immunoassays (ELISA) is predominantly the speed with which results are obtained, roughly two and a half hours. However, the high cost per single test may necessitate batching of samples. It also requires an ELISA reader, which is very expensive. Moreover some enzyme immunoassays (EIA) do not help to discriminate between toxigenic and non-toxigenic C. difficile association, as it detects a non-toxic marker enzyme i.e. glutamate dehydrogenase. A high percentage of indeterminate readings also add up to the mess. Because of lack of confidence of EIA for C. difficile , some clinicians assume an initial negative result may represent a false negative test and repeat the stool testing. EIA has sensitivity and specificity ranges of 50 to 90% and 70 to 95% respectively. About 100 to 1000 pg of toxins must be present for the test to be positive Most ELISA assays have a sensitivity of more than 80% compared to that of tissue culture assay. However, ELISA that detect only toxin A may miss out on toxins from isolates of A - B + strains and thus result in wrong interpretation. Thus, ELISA that detect both toxin A and B are recommended to detect these atypical isolates. Such tests will also take care of specimens containing low levels of toxin A and B. (v) Latex agglutination test: Commercially available latex agglutination test (LAT) is rapid, but is unaffordable for routine use because of the high cost per test. Moreover commercially available LAT is known to detect a non-toxic marker antigen for C. difficile just as the enzyme immunoassays and therefore frequently results in false positive reactions. (vi) Rapid membrane tests : These are lateral flow devices with colored conjugates or flow through formats that require multistep processing. Such tests utilize peroxidase tagged antibodies and a wash step followed by the addition of a substrate. The sample preparation for these tests requires centrifugation or filtration. These tests have sensitivity in the range of 60 to 89%. These tests are toxin A specific and therefore they do not detect A - B + isolates. (vii) Polymerase chain reaction : The polymerase chain reaction (PCR) primers amplify a repetitive sequence of the enterotoxin gene or toxin B in isolates or faeces thereby generating a distinctive ladder pattern. The detection technique is more sensitive than standard culture and has sensitivity similar to cytotoxin testing. The most important advantage of PCR is the rapidity that it offers for pathogen diagnosis. But the great drawback with PCR is that it needs appropriate infrastructure and technical expertise. They are also coupled with time-consuming post PCR manipulations for analysis of the amplification products i.e., agarose gel electrophoresis and Southern hybridization. Most of these assays target only one of the two genes, potentially missing strains carrying only one of them. PCR inhibitory components found in faeces can also cause difficulties in the assay. Moreover, PCR detects even minute number of C. difficile genome copies present even in healthy individuals thereby overemphasising the aetiology. (viii) Immunochromatography assay: The immuno-chromatography technique is a single test enzyme immunoassay for detection of toxins A and B in faecal samples. It can be done within 20 minutes and without any requirement of pre-treatment. (ix) Loop mediated isothermal amplification: Loop mediated isothermal amplification (LAMP) is a rapid and simple method for detecting toxin B gene in stool samples as well as in isolates. Detection of tcdB by LAMP from overnight cultures in cooked meat medium could be an alternative method of diagnostic testing at clinical laboratories without special apparatus but is not as sensitive as the PCR, though easier to perform. (f) Serotyping: The serotyping of each C. difficile strain can be done by ELISA. Polyclonal antisera can be used corresponding to the commonly observed serotypes (i.e. A1, A5, A8, A9, A10, B, C, D, F, G, H, I, K, X and S). Most serotypes belonging to A, C, G, H, and S are considered toxinogenic. However initial culturing for recovery of isolates would be required. This approach would be useful for epidemiological typing. There exist many methods to type or fingerprint strains of C. difficile for outbreak investigations and epidemiological purposes, like serotyping bacteriophage typing, bacteriocin ribotyping, radiolabelled methionine polyacrilamide gel electrophoresis, immunoblotting, restriction enzyme analysis and restriction fragment length polymorphism. Some of these phenotypic and genotypic methods have generated collective evidence in an International Typing Study that there are more types of C. difficile in existence than were previously recognised. Therapy and Management Early resolution of the diarrhoeal symptoms even in some cases of established PMC is most often achieved by withdrawal of the antibiotic therapy that precipitated the disease or at least changing antibiotic regimens. Attention to fluid replacement and electrolyte balance is also necessary. About 25% of patients respond within a few days to these simple measures. In case of non-response they should be treated with specific antimicrobial therapy, which is crucial to prevent the progression of C. difficile pathogenesis. Oral vancomycin is the drug of choice for seriously ill patients with PMC because it has no side effect and is not absorbed by the gut wall. Nearly all patients respond to treatment and diarrhoea resolves over an average of 5 days. However, 5-25% relapse rate may occur after vancomycin treatment. Vancomycin is also the drug of choice for the rare case of Staphylococcal enterocolitis when PMC is proven but C. difficile is undetectable by laboratory tests. The bitter taste of vancomycin can be avoided by prescribing capsules rather than oral suspension. However, oral suspensions are preferable to achieve high concentrations in the colon more quickly in seriously ill patients. In patients too ill for oral therapy, vancomycin, has been administered by nasogastric tube, a long intestinal tube, by enema, or by direct instillation through a colostomy or ileostomy. Intravenous vancomycin can be given to patients who are unable to take oral medication with the hope that some of the drug will reach the colonic lumen through the inflamed mucosal surface. But these desperate measures are not reliable and patients who continue to do poorly may even require caecostomy or colectomy. Relapses occur approximately 20% of the time and some patients have a series of relapses, extending the illness. The routine use of vancomycin has been discouraged because of cost and the potential development of vancomycin-resistant enterococci. Therapeutic alternative to vancomycin is oral metronidazole which is favoured sometimes because it is less expensive. Randomized trials show excellent initial responses in approximately 95% of patients treated with metronidazole. But, the disadvantage of the drug is the near complete absorption such that the levels achieved in the colon are virtually nil. Some isolates of C. difficile are resistant to metronidazole. Metronidazole therefore is used for patients with PMC who are mildly or moderately ill but not for critically ill patients. Ampicillin, although highly active against C. difficile , is largely inactivated in the colon by b-lactamase producing organisms. Oral bacitracin has also been used successfully to treat acute PMC. However, it is significantly expensive and often unavailable and has a very unpleasant taste. Some strains of C. difficile are also resistant to bacitracin. Other antibiotics like fusidic acid and teicoplanin have been tried with little success. The recent changes in the severity of CDAD have stimulated the search for better treatment options. C. difficile shows good in vitro susceptibility to various antimicrobials, such as rifaximin, ramoplanin and nitazoxanide and could be used in future trials. Patients respond rapidly to antimicrobial therapy, but since the therapy kills the normal bacterial flora, it can also cause the disease to recur. Once the colon has been injured, it seems to be more susceptible to reinfection. Other therapeutic methods employed from time to time with limited success are administration of intravenous gamma globulin and microbial interventions using Lactobacilli species or Saccharomyces boulardii to replace the offending C. difficile flora. Even rectal instillation of fresh stool in saline from living related donors and rectal instillation of mixed broth cultures of stool flora have been tried to replenish the normal flora. Cholestyramine and other ion exchange resins like cholesterol or Isabgol husk have been used as binding agents for C. difficile toxin. Tolevamer, a toxin binding polymer is also under investigation as a 'decoy toxin receptor'. However, it should be realized that they may also bind vancomycin when administered and at the same time prolong the symptoms by delaying elimination of toxins. There is a strong association between serum antibody responses to toxin A and protection against C. difficile diarrhoea. Vigorous serum anti-toxin A antibody responses develop in healthy adults by parenteral administration of C. difficile toxoid vaccine. There is a feasibility that such a vaccine might protect high risk individuals against CDAD. Management of CDAD in the community Patients with mild to moderate CDAD in the community can be managed as out patients by the following measures:
Prevention and Guidelines for Infection Control Measures Several measures significantly reduce the incidence of CDAD. The disease can be prevented and/ or controlled when following procedures are implemented:
Conclusion CDAD is thus the most common enteric infection encountered in hospitals and nursing homes with significant medical and economic consequences. The infection spreads quickly because it is very difficult to eradicate the spores from the wards. The spores of C. difficile can persist in dormant state for months together providing a reservoir for new infections. The infected host - either as a patient or as an asymptomatic carrier - may further help to disseminate the disease in susceptible individuals. It is not easy to eliminate the spores from high-risk environments as they are resistant to heat and standard disinfectants. As hospitalised patients with diarrhoea disseminate the infection, hospital personnel involved in patient care become vehicles of perpetuation and spread of the disease. Hospitalised patients receiving antibiotics for ailments are at great risk of acquiring CDAD. Because of the impossibility of eradicating spores from the environment and difficulty of the gut flora to re-establish in the antibiotic environment, CDAD can relapse or recur. However, apart from this, community acquired CDAD signals the threat of several risk factors other than antibiotics. The emergence of a hypervirulent C. difficile strain circulating globally has set alarm bells ringing. The number of established and potential risk factors is being increasingly identified and therefore it is very difficult to say which factor contributes the most to increased CDAD risk. Thus it becomes important to identify the predominant risk factors associated with CDAD. Management of risk factors by infection control education, training and practice and finally by regular audit is required to contain the global epidemic. Treatment should not be based on length of hospitalisation but rather on the presence of clinically significant diarrhoea with a history of antibiotic therapy or the presence of acute abdominal syndrome with little or no diarrhoea. Patient management becomes difficult as culture of the isolates, toxin assays and genetic subtyping, are not routinely available. However, wherever possible the final interpretation of results must be established on the basis of physician's experience and clinical relevance, considering the age of the patient, looking for an history of antibiotic exposure, history of diarrhoea, presence of C. difficile toxin and adequate quantity of faecal lactoferrin as well as absence of other intestinal pathogens. Infection control plays a key role in controlling CDAD outbreaks. The spores of C. difficile can lurk in the hospital environment for months, providing a reservoir for new infections. Active and aggressive surveillance activity is the key to reduce incidence of CDAD. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09087f4.jpg] [mb09087f2.jpg] [mb09087f3.jpg] [mb09087f1.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}