 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 329-334 Original Article Anti - microbial resistance stratified by risk factor among Escherichia coli strains isolated from the urinary tract at a rural clinic in Central India *B Chatterjee, S Kulathinal, A Bhargava, Y Jain, R Kataria Jan Swasthya Sahyog, (CB, BA, JY, KR) Village and P. O. Ganiyari - 495 112, District Bilaspur, Chhattisgarh, India; and Indic Society for Education and Development (KS), 1 Swami Enterprises Complex, Tigrania Road, Tapovan Bridge, Nashik - 422 011, Maharashtra, India Correspondence Address: *Jan Swasthya Sahyog, (CB, BA, JY, KR) Village and P. O. Ganiyari - 495 112, District Bilaspur, Chhattisgarh, India, doctorbiswaroopchatterjee@gmail.com Date of Submission: 11-Feb-2009 Code Number: mb09093 PMID: 19736402 DOI: 10.4103/0255-0857.55449 Abstract Background: The failure of empirical therapy is frequently observed, even in community-acquired urinary tract infections. We, therefore, conducted a prospective, clinic-based study in 2004-2005 to document anti-microbial resistance rates and correlate them with possible risk factors to assist empirical decision-making.Materials and Methods: Symptomatic patients with pyuria underwent urine culture. Isolates were identified using standard methods and anti-microbial resistance was determined by disk-diffusion. Ultrasonography was used to detect complicating factors. Patients were stratified by the presence of complicating factors and history of invasive procedures for comparison of resistance rates. Statistical Method Used: Chi-square or Fisher exact tests, as appropriate. Results: There were 156 E. coli isolates, of which 105 were community-acquired. Twenty-three community-acquired isolates were from patients with complicating factors while 82 were from patients without any. Fifty-one isolates were from patients who had recently undergone invasive procedures on the urinary tract. Thirty-two community-acquired isolates from reproductive-age women without apparent complicating factors had resistance rates of 50% or above against tetracyclines, Co-trimoxazole, aminopenicillins, Nalidixic acid, Ciprofloxacin and 1 st generation cephalosporins. Resistance rates were significantly higher among isolates from patients subjected to invasive procedures, except against Co-trimoxazole, tetracyclines and Amikacin. Conclusion: High rates of anti-microbial resistance in community-acquired uropathogens have made antimicrobial sensitivity testing necessary even in a rural, primary-care setting. Keywords: Antimicrobial resistance, E. coli, urinary tract infection Introduction Urinary tract infections (UTIs) are one of the commonest bacterial infections and a single species, Escherichia coli , accounts for majority of these. [1],[2] Community-acquired strains of E. coli causing UTI in the absence of complicating factors such as obstruction, calculi, anatomic anomalies, reflux etc. often belong to successful uropathogenic clones that possess adhesins, siderophores, haemolysins and other virulence factors that facilitate colonisation and infection. [3] Some of these strains have also been found to carry integrons with genes that mediate multiple antimicrobial resistance. [4] Strains of E. coli that infect patients with complicating factors or a history of invasive procedures on the urinary tract, may lack specialized virulence factors. Anti-microbial resistance rates of these latter strains vary and are highest among nosocomial strains under intense selection pressure in the hospital environment. In the course of our work in central India, with a predominantly rural population that has poor access to healthcare, we have seen failure of empirical treatment of community-acquired UTIs with commonly-used, orally-administered drugs in more than a third of cases. This happens regardless of the presence of complicating factors. Failure of empirical treatment of nosocomial UTI occurs even more frequently. The aim of the present study was to document resistance patterns of E. coli responsible for urinary tract infections in our area. We compared resistance rates between community-acquired isolates from patients with or without complicating factors and between community-acquired and hospital-acquired isolates to look for possible differences that could aid clinical decision-making while awaiting laboratory test results. In particular, we looked at community-acquired UTI in reproductive age-group women without apparent complicating factors, since they comprise the commonest subset of UTI patients in an outpatient setting. Materials and Methods Subjects The subjects of the study were 356 consecutive outpatients and inpatients with symptoms suggestive of urinary tract infection during the 12-month period from October 2004 to September 2005. Dysuria, frequency, urgency, strangury and suprapubic discomfort were defined as symptoms of cystitis, while low-back pain or flank pain, fever, nausea and chills were defined as symptoms of pyelonephritis for the purpose of the study. Methods The study and data collection were carried out with approval from the Institutional Ethics Committee. Informed consent was taken from all subjects. Symptomatic subjects underwent physical examination and urine microscopic examination. For uniformity, 15-ml of well-suspended urine was centrifuged at 2,000 rpm for 10 minutes. The deposit was re-suspended in a volume of 200-μl, of which 50-μl was deposited on a microscope slide and covered with a 22 x 22 mm cover slip. Since this is tantamount to concentrating the microscopic elements in urine 75-fold (15,000 μl / 200 μl), we defined significant pyuria as 10 or more pus cells per high power (400x) field by multiplying 75-fold the lower limit of significant pyuria of 1 leucocyte per 7 HPF in uncentrifuged urine. [5] Fresh urine samples for bacterial culture were obtained by proper technique from patients with significant pyuria. Most samples were processed within two hours of reception. When this was not possible, samples were stored for a maximum duration of 24 hours on wet ice pending inoculation. [6] 10 μl of well-suspended urine was plated on CLED agar using disposable loops. Plates were incubated at 35°C for up to 48 hours. A positive culture was defined as the isolation of bacteria in pure culture with a colony count of at least 104 colonies per ml. [3] Attempts were made to identify isolates by standard methods. [7],[8] E. coli, in particular, was identified as follows: Non-fastidious (grew on CLED), glucose-fermenting (acid butt in TSI) and oxidase-negative, Gram-negative bacilli (presumptively Family Enterobacteriaceae) were further considered for possible identification as E. coli . Isolates that were citrate-positive, VP-positive, hydrogen sulphide-positive, urease-positive, or phenylalanine deaminase-positive were excluded from consideration. Isolates that scored negative for all the previous biochemical tests were scored for the following tests: indole production, methyl red positivity, mannitol fermentation, and lysine decarboxylation. Isolates that scored positive in at least three out of the latter four tests were reported as E. coli. Lactose fermentation, motility and gas production did not play a role in our decision-making process because of the extreme variability of these characteristics in E. coli. Resistance to aminopenicillins, first and third generation cephalosporins, Gentamicin, Amikacin, Nalidixic acid, Ciprofloxacin, Nitrofurantoin, Chloramphenicol, Doxycycline, and Co--trimoxazole (and other drugs as appropriate for other isolates) was tested by the Kirby-Bauer technique according to guidelines of the erstwhile National Committee for Clinical Laboratory Standards (NCCLS), using E. coli ATCC 25922 as control. [9] The production of extended-spectrum beta--lactamases (ESBL) was not looked at in this study. The cost of culture and ultrasonography was borne by the organisation and not passed on to study subjects. Patients with positive cultures were questioned for a history of invasive procedures on the urinary tract in the past six months. Female patients less than two years or more than 50 years of age and all male patients underwent ultrasonography (USG) for detection of complicating factors such as anatomic anomalies, obstruction or calculi within a week of presentation. We did not perform USG for symptomatic women in the reproductive age group because underlying structural abnormalities occur in only about five per cent of cases of acute pyelonephritis in this subgroup. [3] Patients were stratified into three risk groups on the basis of complicating factors and a history of invasive procedures, as follows:
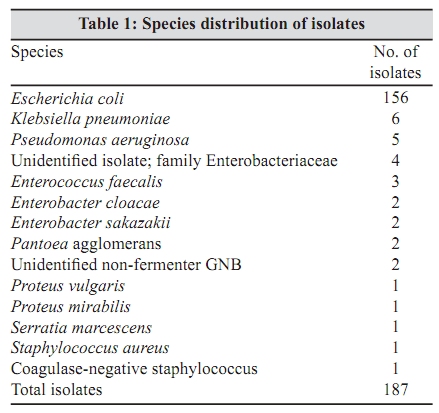
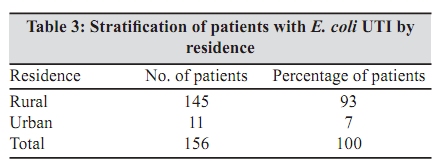
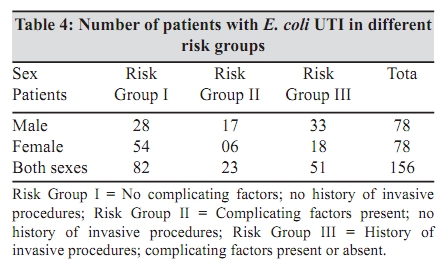
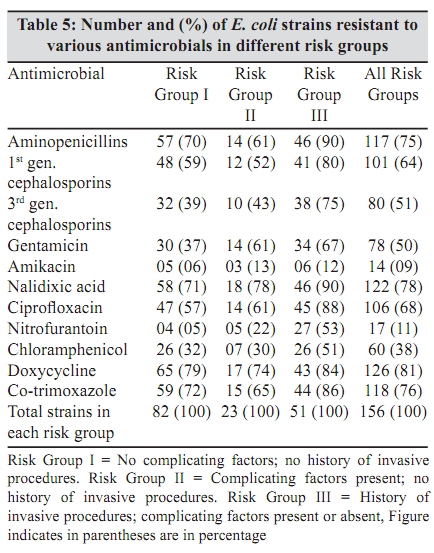
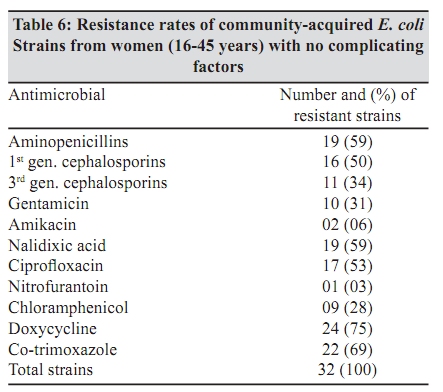
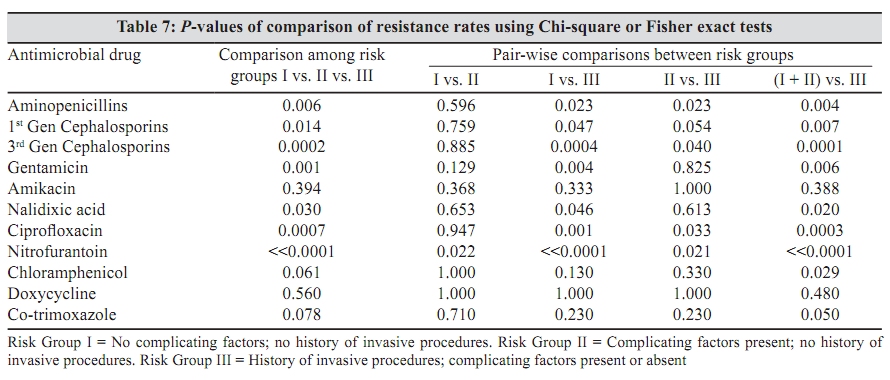
Although we had initially planned to look at a history of prior anti-microbial treatment (especially improper dose and duration of treatment) as a possible risk factor for drug resistance, we gave up after we realised that many patients are treated in villages by unqualified practitioners without prescriptions, making it impossible to acquire a dependable antimicrobial history. Statistical analysis Chi-square test was used to assess differences in resistant rates between the three groups. Yates correction for continuity was used for pair-wise comparisons after correcting for multiple testing by Bonferroni inequality. Fisher's exact test was used when the number of strains in any group was less than five. For both tests, P -value below 0.05 was considered statistically significant. Statistical analyses were performed using R statistical computing software. Results There were 356 symptomatic patients, out of whom 241 had pyuria and underwent urine culture. Culture was positive in 187 patients. Identical isolates from the same patient were not considered for analysis. One hundred and fifty-six isolates were E. coli , accounting for 83% of all isolates [Table - 1]. There were 78 male and 78 female patients with E. coli UTI. Comparatively, more male patients lay at the extremes of age [Table - 2]. Ninety-three percent of patients came from villages [Table - 3]. We stratified patients with E. coli UTI into three risk groups on the basis of complicating factors and a history of invasive procedures on the urinary tract. Female patients predominated in Risk Group I with no complicating factors and no history of invasive procedures, while male patients predominated in Risk Group II (complicating factors present) and Risk Group III (history of invasive procedures on the urinary tract) [Table - 4]. The number and percentage of E. coli strains resistant to different antimicrobials from each risk group is given in [Table - 5]. In all risk groups, 50% or more isolates were resistant to Co--trimoxazole, tetracyclines, aminopenicillins, first t generation cephalosporins, Nalidixic acid and Ciprofloxacin, while approximately 30% or more isolates were resistant to Chloramphenicol, Gentamicin and third generation cephalosporins. The lowest resistance rates were seen against Amikacin. Putative nosocomial isolates in risk group III had higher rates of resistance against most antimicrobials compared to community-acquired isolates in risk groups I and II. One of our nosocomial strains was resistant to all of these drugs and was sensitive only to Piperacillin--Tazobactam and carbapenems (data not presented in table). [Table - 6] gives the anti-microbial resistance rates of E. coli strains isolated from a subset of Risk group I patients, namely reproductive age-group women without apparent complicating factors and no history of invasive procedures on the urinary tract. Data for this subset is presented separately as it comprises the largest number of UTI patients in the community. [Table - 7] gives P -values of comparison of rates of resistance against different antimicrobials, i) among all the three risk groups, ii) between each possible pair of risk groups, and iii) between combined risk groups I plus II (community-acquired isolates) and risk groups III (isolates likely to be of nosocomial origin). Discussion In our series, 105 out of 119 (92%) community-acquired isolates and 51 out of 68 (66%) putative hospital--acquired isolates were E. coli . This tallies with a study from Srinagar, Kashmir where 90% of the isolates from unstratified patients in a primary healthcare setting were E. coli . [10] Our findings, however, contrast markedly with those of a study from Chandigarh, where E. coli comprised 64% of 602 outpatient isolates and 46% of 808 inpatient isolates respectively. [11] This difference possibly arose from the differences in patient profiles between our centre that provides primary and secondary level care and Government Medical College, Chandigarh that provides secondary and tertiary level care. Among our 32 E. coli strains from reproductive age-group women, who had no complicating factors and had not been subjected to invasive procedures, resistance rates below 10% were seen only against Amikacin and Nitrofurantoin. It is noteworthy that 31% of these isolates were simultaneously resistant to five orally-administered agents that are most often used for the treatment of UTI in an outpatient setting, namely aminopenicillins, first generation cephalosporins, Co--trimoxazole, Nalidixic acid and Ciprofloxacin. Comparison of these isolates with 59 isolates obtained from antenatal and postnatal women at CMC, Vellore in 2002 shows similar resistance rates for aminopenicillins (59 at our centre vs. 52% at Vellore), Co-trimoxazole (69 vs. 58%), and Amikacin (six vs. five per cent). However, resistance rates to Ciprofloxacin (53 vs. 22%), third generation cephalosporins (34 vs. 10%) and Gentamicin (31 vs. 19%) were higher at our centre while resistance to Nitrofurantoin (03 vs. 11%) was seen more frequently in Vellore. [12] Among our community-acquired E. coli isolates, there was no significant difference in resistance rates between patients in Risk Group I (complicating factors absent) and patients in Risk Group II (complicating factors present), except against Nitrofurantoin. We, therefore, combined Risk Groups I and II and compared them with Risk Group III isolates, which were presumably hospital--acquired as they came from patients, who had recently undergone an invasive procedure on the urinary tract. E. coli isolates from patients in Risk Group III were found to have significantly higher rates of resistance against most antimicrobials tested. Six of our hospital-acquired isolates were simultaneously resistant to all penicillins, cephalosporins, aminoglycosides and fluoroquinolones but four of these were sensitive to Nitrofurantoin, offering an affordable treatment option, Comparison of 51 E. coli isolates in patients with a history of invasive procedures on the urinary tract at our centre with 58 E. coli isolates from urology patients at Christian Medical College, Vellore in the year 2002 showed similar rates of resistance with a significant difference found only against Amikacin (12% at our centre vs. 35% at Vellore). [12] These high resistance rates in uropathogenic isolates from a predominantly rural population with poor access to healthcare raises questions about the selection pressures that generate and maintain resistance and the factors that allow resistant strains to spread in the community. It is possible that irrational prescription of anti-microbials, available over-the-counter (OTC) in India, has contributed to this situation. Unqualified practitioners and untrained pharmacists all over the country use antimicrobials indiscriminately and often in non-standard doses for inadequate durations. [13] Similar practices have been reported from other developing countries, including Nepal and Vietnam. [14],[15] The widespread use of antimicrobials in veterinary practice is another possible factor fuelling the emergence of resistant strains. The isolation from cattle of drug-resistant E. coli clonal group A strains, an important cause of UTIs, lends support to this possibility. [16] In the past decade, several publications have suggested novel routes for the spread of drug--resistant, uropathogenic E. coli clones. There is evidence that in many patients with E. coli UTI, the uropathogenic clone colonizes the large intestine. [17] Just like any other E. coli strain, uropathogenic E. coli clones can be excreted in faeces and carried in water to be ingested by other people and colonize the large intestine, from where they can initiate urinary tract infection in the new host. In fact, E. coli clones that possess genes for uropathogenic virulence factors, have been found in waste-water and food. [18],[19] Although these studies have come from western countries, there is every likelihood of uropathogenic E. coli spreading through faecal contamination of groundwater in rural India where sanitation facilities are scarce. Finally, uropathogenic E. coli strains have also been shown to be shared between sexual partners. [20] High resistance rates in nosocomial strains are typically engendered by the intense selection pressure in the hospital environment. These strains are known to be spread between patients through contaminated equipment as well as the hands of healthcare personnel. [21] To conclude, the study demonstrated 30 to -50% resistance rates in uropathogenic E. coli in a rural area to most antimicrobials that are commonly used in a primary and secondary healthcare setting. Amikacin and Nitrofurantoin were the only drugs tested against which resistance rates of community--acquired isolates were less than 10%. The aim of the study to find clinical predictors of resistance resulted in the identification of nosocomial source as the major identifiable risk factor. Nosocomial infections were practically untreatable with affordable antimicrobials without the benefit of laboratory testing. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09093t3.jpg] [mb09093t4.jpg] [mb09093t5.jpg] [mb09093t1.jpg] [mb09093t7.jpg] [mb09093t6.jpg] [mb09093t2.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}