 |
| About Bioline | All Journals | Testimonials | Membership | News |
|
||||||
|
||||||
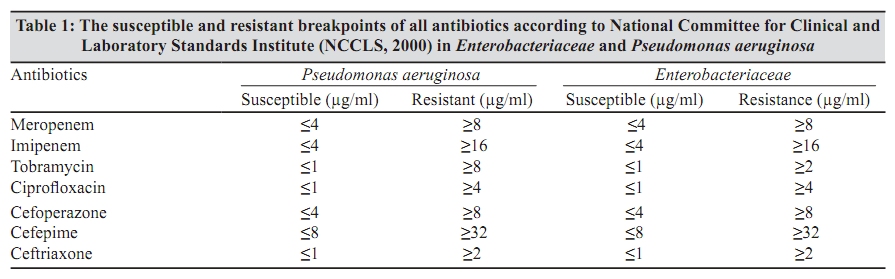
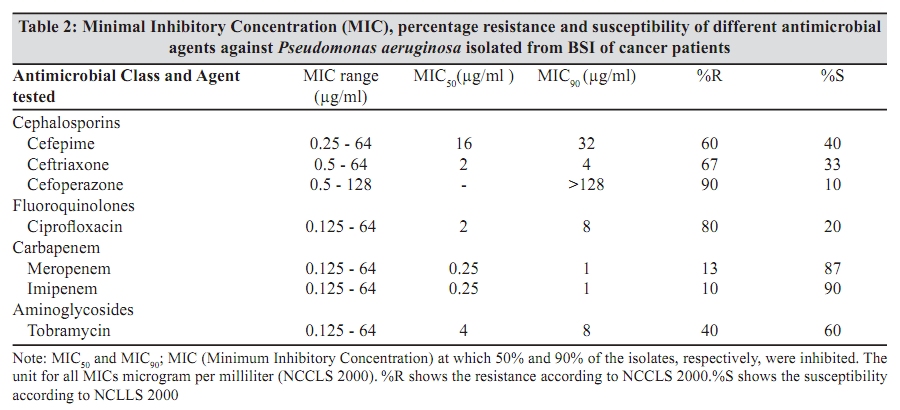
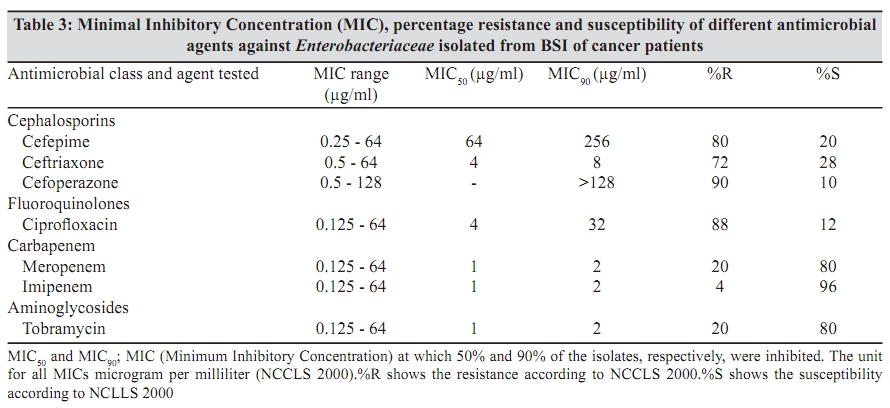
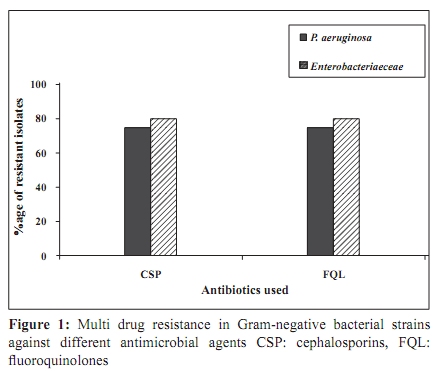
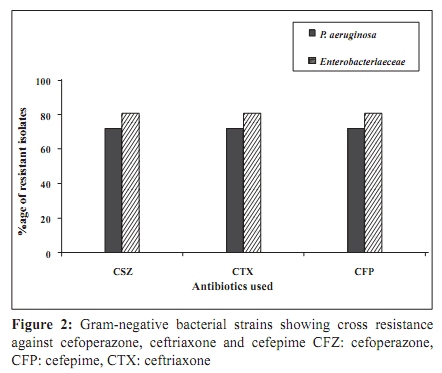
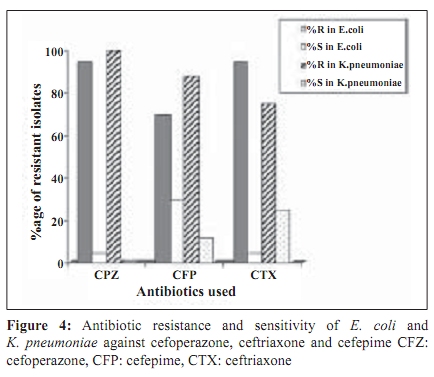
Indian Journal of Medical Microbiology, Vol. 27, No. 4, October-December, 2009, pp. 341-347 Original Article Characterization and anti - microbial susceptibility of gram - negative bacteria isolated from bloodstream infections of cancer patients on chemotherapy in Pakistan *S Saghir, M Faiz, M Saleem, A Younus, H Aziz Institute of Biochemistry and Biotechnology (SS,MS,AY), University of the Punjab, Lahore, Pakistan, Institute of Nuclear Medicine and Oncology (INMOL) (MF,HA), Lahore, Pakistan Correspondence Address: *Institute of Biochemistry and Biotechnology, University of the Punjab, Lahore, Pakistan, syra.akif@gmail.com Date of Submission: 23-Oct-2008 Code Number: mb09095 PMID: 19736404 DOI: 10.4103/0255-0857.55454 Abstract Purpose: Bloodstream infection remains a major cause of morbidity and mortality in patients undergoing treatment for cancer. Severe infections due to Gram-negative bacilli & staphylococci are common in cancer patients. Altered gut flora because of frequent antibiotic administration and damage of epithelial surfaces contribute to the development of infection. To access the use of new potent antibiotics against bloodstream infection in cancer patients and to determine the cross resistance of Gram-negative bacterial strains.Materials and Methods: We studied the bacterial spectrum & antimicrobial susceptibility pattern of cephalosporins, fluoroquinolones, carbapenems and aminoglycosides against Gram-negative bacterial strains in cancer patients. The susceptibility was determined by broth dilution method according to National Committee for Clinical Laboratory Standards (NCCLS) now called Clinical Laboratory Standards Institute (CLSI) during study period (July 2006 to Jan 2007). Results: A total of 60 Gram-negative bacterial blood cultures were examined. Among these, Pseudomonas aeruginosa was the most common (38%). The Minimum Inhibitory Concentration at which 50% (MIC 50 ) and 90% (MIC 90 ) of Enterobacteriaceae and P. aeruginosa inhibited were found. Resistance in P.aeruginosa against cefepime, meropenem, ciprofloxacin, ceftriaxone, tobramycin, cefoperazone and imipenem was 60%, 13%, 80%, 67%, 40%, 90% and 10% respectively while for Enterobacteriaceae 80%, 20%, 88%, 72%, 20%, 90% and four per cent resistance was observed. Meropenem was found to be the most effective antimicrobial against Gram-negative bacteria. Conclusion: High resistance observed in this study warrants the needs of surveillance of resistant pattern of antimicrobial agents. Due to increased level of drug resistance, carbapenem would be a prudent choice in high- risk cases. Keywords: Bloodstream infection, Cancer patients, Enterobacteriaceae, Gram-negative bacteria, Pseudomonas aeruginosa Introduction Infection is a continuous and significant problem in patients with cancer. Cancer causes both direct and indirect effect on a patient's immune system. Many factors increase the susceptibility of immunosuppressed cancer patients to infection. These include neutropenia during aggressive therapy, altered gut flora because of frequent antibiotic administration, disruption of skin and damage of epithelial surfaces by cytotoxic agents. Bloodstream infection (BSI) is a leading infectious complication among cancer patients and has a negative impact on patients' outcome. These infections are being reported as a leading cause of morbidity and mortality worldwide. Moreover, BSI represents about 15% of all nosocomial infections. [1] BSIs due to Gram-negative bacilli are common in cancer patients during aggressive therapy. In recent years, there has been marked increase in the incidence of antibiotic resistance against Gram-negative bacilli. [2],[3] The overall frequency of Gram-negative infection has decreased over the past decade, but data from several large surveillances studies conducted at major cancer centers both in the United States and Europe indicate that Enterobacteriaceae cause approximately 65% to 80% of documented Gram-negative infections in these patients. However, Pseudomonas aeruginosa is also associated with significant morbidity and mortality in immunocompromised hosts. The purpose of this study was to determine the antimicrobial susceptibility of bacterial clinical isolates and determine the frequency of Gram-negative bacteria like Pseudomonas aeruginosa and Enterobacteriaceae causing bloodstream infection in cancer patients. This need was increasing with increasing resistance and the emergence of multidrug-resistant microorganisms. Testing is required not only for therapy but also to monitor the spread of resistant organisms or resistance genes throughout the hospital and community. Similarly, as observed in routine analysis, resistance to number of drugs like cephalosporins, fluoroquinolones, carbapenems and aminoglycosides was also increasing. The aims and objectives of the present study were to determine the antimicrobial and cross resistance of different antimicrobials used for treating infections in cancer patients. This study helped assess the new potent antibiotics and current resistance pattern against several drugs being used in cancer treatment. Materials and Methods Selection of patients The study was carried out at Microbiology Laboratory of Institute of Nuclear Medicines and Oncology, Lahore (INMOL), over a period from July 2006 to Jan 2007. All hospitalized cancer patients undergoing anti-cancer therapy, with suspected blood stream infection, were studied. No discrimination was made on the basis of age or gender. Patients already undergoing anti-microbial therapy and those having fever due to non-infectious causes such as blood transfusion and drug infusion etc., were excluded from the study. Only one isolate per patient was studied at a time and total blood samples were taken for analysis. Media preparation for culturing Different culture media like nutrient broth, nutrient agar, blood agar, Muller Hinton broth (Oxoid Limited, Wade Road Basingstoke, UK) MaConkey agar (Biozyme Laboratories Ltd, Hibert Street, Suite 101 San Diego, USA) and Brain heart infusion broth. (Oxoid Limited Wade Road Hampshire, UK) were used for isolation and culture of micro-organisms. Identification, characterization and culture condition of Bacterial strains A total of 60 Gram-negative isolates were studied at Institute of Nuclear Medicine and Oncology (INMOL) Lahore, Pakistan. Isolation by adding about five ml blood obtained from peripheral veins of the patients to nutrient broth was done. The blood culture bottles were incubated at 37°C up to a week. To obtain well-isolated colonies, the inoculums were spread on the surface of an enriched agar plate to obtain single colony and incubated at 37 degree celsius for 24 hours. Each strain was named on the basis of morphology of the colony, gram staining and biochemical characterization. The plates containing purified strains were stored at 4°C. Standard biochemical tests (oxidase test, citrate utilization test, indole test, urease test and Kligler iron agar test) performed according to Manual of clinical microbiology [4] helped in further identification of bacterial samples. Bacterial samples were stored as glycerol stocks at -20°C till further use. Antimicrobial agents Three groups of antibiotics were studied. Carbapenem (Meropenem, Imipenem), Cephalosporin (Ceftriaxone, Cefepime and Cefoperazone) and Amino glycosides (Tobramycin) obtained from local pharmaceutical companies (Bristol- Myers Squibb S.P.A Italy and P & S- Partner GmbH, Germany) for the antimicrobial sensitivity testing. All the stock solutions of pure antibiotics were prepared in sterile distilled water or as specified by the manufacturer's recommendations. Different dilutions were prepared for Minimum Inhibitory Concentration (MIC) determination Sensitivity studies and Minimum Inhibitory Concentration (MIC) Inoculums were prepared, by inoculating single purified colonies of bacterial and control strains into Muller Hinton Broth (Oxoid Limited, Wade Road Basingstoke, UK), and incubated overnight at 37ºC. Optical density was measured with a Spectrophotometer at 546 nm (Bibby Scientific Limited, Jenway and Essex, UK). The density of the inoculum was adjusted 10 5 Colony Forming Unit/ml and used in MIC determination . Minimum Inhibitory Concentration (MIC) was determined in duplicate in Muller Hinton Broth containing serial two-fold dilutions of each antibiotic with inoculated bacterial suspensions of 10 5 CFU/ml as outlined by the National Committee for Clinical Laboratory Standards [5] The results were recorded after overnight incubation at 37ºC. The MIC was defined as the lowest antibiotic concentration with no visible growth. The MIC 50 and MIC 90 were defined as minimum concentration of antimicrobial that inhibited 50% or 90% of the isolates, respectively. The NCCLS susceptible and resistant breakpoints of ciprofloxacin, ceftriaxone, tobramycin, meropenem, cefepime, cefoperazone and imipenem were showed in [Table - 1]. Detection of Extended-spectrum beta-Lactamase (ESBL) production ESBL activity was detected by demonstrating the loss of activity of a beta lactam agent against a susceptible indicator organism. The method for detection of ESBL activity was based on the recommendation of National Committee for Clinical Laboratory Standard (NCCLS). All isolates resistant to cephalosporin (ceftazidime, ceftriaxone, cefotaxime) were tested for ESBL production according to the required method [6] Discs containing cefotaxime and ceftazidine 30 µg are applied to the medium either side of one containing amoxicillin and clavulanate (20 plus 10µg) and 25-30 mm away from it. Inoculated media were incubated for 18-24 hours at 37°C. Enhanced zone of inhibition between any of the beta- lactam discs and the center disc was recorded. [7] ESBL production was inferred when the zone of either cephalosporin is expanded by clavulanate. Zone diameter within the grey zone was considered as a probable ESBL positive strain. K. pneumoniae and E. coli were frequently used for the detection of the ESBL activity. E. coli and K. pneumoniae strains on Muller Hinton medium showing ESBL activity in Muller Hinton medium. Data Analysis The data was analyzed and evaluated on the basis of averages and percentage values. The results were presented in the form of tables, figures and graphs. Results Frequency of occurrence of bacterial pathogens A total of 60 Gram-negative bacteria, collected and studied from July 2006 to Jan 2007 were characterized on the basis of oxidase test, indole test, urease test, citrate test and KIA test. Among Gram-negative bacteria, Pseudomonas aeruginosa (38%) was the most frequently isolated bacterial strain followed by E. coli (25%), Klebsiella (20%), Proteus (10%) and Shigella (7%) Minimum inhibitory concentration against P. aeruginosa The anti-microbial activity of cephalosporins, carbapenems and fluoroquinolones, and aminoglycosides group of antimicrobial agents against P. aeruginosa isolates from bloodstream infection of cancer patients is shown [Table - 2],[Table - 3] .Among all the antimicrobials used, imipenem and meropenem showed highest In vitro activity against Pseudomonas aeruginosa strains. The MIC 50 of meropenem was 0.25 µg/ml and ranged between 0.125-64 µg/ ml. According to NCCLS, susceptibility breakpoint of one µg/ml, 95% of P. aeruginosa isolates were found sensitive [Table - 3]. Among cephalosporins, ceftriaxone has highest In vitro activity. The MIC 50 and MIC 90 of ceftriaxone were found at two µg/ml and four µg/ml respectively. Cefepime have a moderate activity against P. aeruginosa with MIC range between 0.25 - 64 µg/ml. However, 90% of isolates were susceptible at a concentration of 32 µg /ml and 50% of isolates were susceptible at 16 µg/ml [Table - 3]. Tobramycin was also found to be effective against P.aeruginosa isolates. P. aeruginosa isolates were found to have less In vitro activity against fluoroquinolones as compared to cephalosporins (ceftriaxone, cefepime and cefoperazone). The In vitro activity of ciprofloxacin was least demonstrating MIC 50 and MIC 90 of two µg/ml and eight µg/ml respectively. A high resistance rate among the test strains was noticed that was even higher than ceftriaxone and cefepime [Table - 2]. The antimicrobials in P. aeruginosa , in decreasing order, were as follows: Imipenem, Meropenem, Tobramycin, Ceftriaxone, Ciprofloxacin, Cefepime, Cefoperazone. Minimum inhibitory concentration determination against Enterobacteriaceae In case of Gram-negative bacteria belonging to Enterobacteriaceae, carbapenem group of antimicrobial agents were found to be more effective compared to cephalosporins, fluoroquinolones and aminoglycosides. The MIC range of meropenem and imipenem was 0.125-64 µg/ml with more than 90% of isolates being susceptible at two µg /ml (NCCLS susceptibility breakpoint) as shown in [Table - 3]. Among cephalosporins, ceftriaxone showed highest in vitro activity with MIC 50 at four µg/ml. However, ceftriaxone was found to be more effective in P. aeruginosa than in Enterobacteriaceae. Cefepime was found to be less effective with MIC 50 at 64 µg/ml [Table - 3]. Activity of cefoperazone against Enterobacteriaceae was found to be least as 90% of strains showed MIC 90 greater than 128 µg/ml [Table - 3]. However, Tobramycin showed good activity as 80% of isolates belonging to Enterobacteriaceae were sensitive. Among fluoroquinolones tested, Enterobacteriaceae isolates were found to have less In vitro activity as compared to cephalosporins (ceftriaxone, cefepime and cefoperazone). The In vitro activity of ciprofloxacin was least demonstrating MIC 50 of two µg/ml as compared to P. aeruginosa [Table - 3]. The activity of different antimicrobial agents in Enterobacteriaceae was found to be - (in decreasing order): Imipenem, Meropenem, Tobramycin, Ceftriaxone, Ciprofloxacin, Cefepime. Cefoperazone. Percentage sensitivity and resistance of Gram-negative bacterial isolates to cephalosporins, carbapenems and fluoroquinolones Looking into the sensitivity and resistance of bacterial strains belonging to Enterobacteriaceae and P. aeruginosa against cephalosporins, carbapenems, fluoroquinolones and aminoglycosides, high resistance was observed in Enterobacteriaceae against cephalosporins. Among cephalosporins, highest resistance was observed in cefoperazone where 90% isolates were resistant. Similarly, about 80% and 70% of isolates were found resistant against cefepime and ceftriaxone respectively [Table - 2]. This resistance pattern is similar in P.aeruginosa strains as 90% of strains were found resistant to cefoperazone followed by cefepime and ceftriaxone where 60% and 67% strains were found resistant respectively [Table - 2]. In ciprofloxacin, more than 80% of strains belonging to Enterobacteriaceae and P. aeruginosa were found resistant whereas sensitivity of strains against ciprofloxacin was only 12% and 20% respectively [Table - 2],[Table - 3]. Ceftriaxone and cefepime were found more resistant in Enterobacteriaceae strains as compared to P. aeruginosa. Among all antimicrobial agents tested, meropenem was found to be more effective. Among bacterial strains belonging to Enterobacteriaceae, 80% strains were sensitive against meropenem whereas in P. aeruginosa , 87% strains were found sensitive against meropenem [Table - 2],[Table - 3]. Multidrug resistance in P. aeruginosa and Enterobacteriaceae strains Multidrug resistance in P. aeruginosa strains isolated in this study was also observed against anti-microbial agents belonging to different groups. About 74% of P. aeruginosa strains showed resistance against both fluoroquinolones, cephalosporins [Figure - 1]. Similarly, about 79% of bacterial isolates of Enterobacteriaceae were found resistant against both fluoroquinolones and cephalosporins [Figure - 1]. Cross resistance in Gram negative bacterial strains P. aeruginosa strains were found highly resistant to single antimicrobial agent, cross resistant to other drugs in this study. More than 72% of strains showed resistance to ceftriaxone, cefepime and cefoperazone. High resistance to all cephalosporins (ceftriaxone, cefepime, and cefoperazone) was also found in Enterobacteriaceae. More than 80% strains showed resistance to all three drug members of the same antibiotic family. [Figure - 2] However, only 12% resistance was found against both meropenem and imipenem in bacterial strains belonging to Enterobacteriacea e, while only 8% strains showed resistance to both meropenem and imipenem [Figure - 3] Determination of antimicrobial resistance of beta Lactamase producers In this study, almost 63% of Gram-negative bacterial isolates belong to Enterobacteriaceae . In this study, Klebsiella (20%) and E. coli (25%) constitute the groups found as beta lactamases producers. Enhanced zone of inhibition between any of the beta- lactam discs and the center disc was recorded. [7] The percentage resistance and sensitivity to cefoperazone, cefepime and ceftriaxone in isolates of E. coli showed that 95% of strains were resistant to ceftriaxone and cefoperazone while 70% were found resistant to cefepime. Similarly in Klebsiella sp., 100%, 88% and 75% were found resistant to cefoperazone, cefepime and ceftriaxone respectively [Figure - 4]. Discussions The potential for anti-microbial resistance is an important concern for clinicians treating patients with confirmed or suspected bacterial infections as they are often resistant to a broad range of antimicrobial agents. Detection of micro-organism in blood culture is considered an indicator of disseminated infection and has been shown to be a valid marker for surveillance of bloodstream infections among critically ill patients. [1] In our study, Gram-negative bacteria was found associated with bloodstream infections in cancer patients. Pseudomonas aeruginosa (38%) was the most frequently isolated bacterial strain followed by E. coli (25%), Klebsiella pneumoniae (20%), Proteus vulgaris (10%) and Shigella (8%). P. aeruginosa has also been reported to cause a wide variety of infections in immunocompromised cancer chemotherapy patients as it is a common hospital and opportunistic pathogen. [2] In our study, imipenem was the most effective drug against Gram- negative bacterial strains. [8] Escherichia coli was the second most common blood culture isolate from hospitalized patients. Reports by SENTRY for laboratories in the United Stated, Canada, Latin America and Europe showed E. coli, Klebsiella sp. and P.aeruginosa as the most frequent resistant bacilli to be isolated from bloodstream infections. [9],[10] The In vitro activity of different anti-microbial agents in Gram-negative bacteria causing BSI was also evaluated in our study. High resistance rates were observed in our study against cephalosporins in both P. aeruginosa and Enterobacteriaceae. [11] In this study, fluoroquinolones, resistance in P. aeruginosa and Enterobacteriaceae against ciprofloxacin was found to be 80% and 88%. High resistance to third generation Cephalosporins and Ciprofloxacin have been reported for Gram-negative Bacilli collected in United States, Canada and Latin America for SENTRY Antimicrobial Surveillance Programmes in Turkey. This high resistance in Enterobacteriaceae was may be due to Beta lactamase activity. [12],[13] Studies on the resistance to ß-lactam antimicrobial agents, especially extended-spectrum cephalosporins and other antimicrobial agents among clinical isolates of Gram-negative bacteria are on the rise worldwide. [14],[15] Numerous reports highlight the increasing importance of Enterobacteriaceae as a cause of bloodstream infection. Fluoroquinolones resistance against E. coli in cancer patients was found with a resistance rate of more than 50% among E. coli. [16] However, low resistance rates has been reported in Gram-negative pathogens of bacteremia in the UK and Ireland between 2001-2002 where resistance rate of P.aeruginosa to ciprofloxacin and ceftazidime was between four to seven per cent. [17] Multidrug-resistance among P. aeruginosa, K. pneumoniae and Enterobacterobacteriaceae species, with emerging resistance, is an important cause of morbidity and mortality in hospitalized critically ill patients and patients with underlying medical condition such as neutropenia and immunosuppressant. In our study, multidrug resistance was also observed among our isolates that is quite concerning. Rate of multidrug resistance was shown to be increased in other reports. [18],[19] Similarly anti-microbial resistance pattern among bloodstream infection isolated from SENTRY antimicrobial Surveillances Program (1997-2002) showed high prevalence of multidrug resistant P. aeruginosa in America. [20] Mortality due to infection with multi drug-resistant P. aeruginosa has growing concern. The lack of alternative agents that are active against gram negative bacteria necessitates the use of measure for controlling emergence of resistance in bacterial strains. Moreover, combination of drugs was found to be the appropriate choice for treatment of P. aeruginosa infections in one study [21] Higher antibiotic resistance is also common feature of beta lactamase producing bacterial strains belonging to Enterobacteriaceae . It was reported that resistance to extended spectrum beta lactamases (ESBL) to the family of Enterobacteriaceae were resistance to cephalosporins. They reported 63% ESBL positive strains. [22] However, in our study, 58% had ESBL positive strain including E. coli, Klebsiella sp. and Proteus. In this study, Klebsiella and E. coli were found more resistant to cephalosporins. Klebsiella was 88% resistant and E. coli was 87% resistant to cephalosporins as compared to other members of Enterobacteriaceae. Positive strains in ESBL were reported and it was found that ESBL producing organisms were resistant to all cephalosporins. [23] Beta-lactam were the most widely used antibiotics against Gram negative bacteria. In our study, resistance to third generation cephalosporins implied extended spectrum beta lactamases (ESBL) production in Escherichia coli and Klebsiella pneumoniae. Hence, beta-lactamases activity produced by Gram- negative bacteria may be the possibility of resistance to cephalosporins studied. Klebsiella (88%), E. coli (87%), Proteus (58%) and Shigella (55%) showed beta lactam resistance. Majority of Klebsiella and E. coli showed high resistance to cephalosporins. [24] In our conclusion, high resistance observed in this study warrants the need for surveillance of resistant pattern of antimicrobial agents administered to patients undergoing treatment for better patient's management. A careful monitoring of anti-microbial use, in hospital, is required to identify the situation in which prescription patterns are contributing to the development of resistance. The lack of any new compounds in the near future indicates that there is need for constant monitoring at national, regional level as these surveillance efforts are essential to provide clinicians with information for choosing empirical treatment regiments and implement strict antibiotic prescribing policies and hospital infection control guidelines. Screening for ESBL production as a routine procedure in clinical laboratories gives valuable information to the clinician in appropriate selection of antibiotics. Moreover, bacterial strains resistant to most classes of antibiotics will continue to arise unless the inappropriate use of these drugs is curtailed. Acknowledgment Scientific Assitance of Dr Mahjabeen Saleem, Miss Mariyum Faiz, Miss Amna Younus and Miss Hafzah Aziz and Technical assistance of Mr Tariq Bashir, Mr Majid, Mr Nawaz, and Mr Ayub is gratefully acknowledged. References
Copyright 2009 - Indian Journal of Medical Microbiology The following images related to this document are available:Photo images[mb09095t3.jpg] [mb09095f2.jpg] [mb09095f1.jpg] [mb09095t1.jpg] [mb09095f3.jpg] [mb09095t2.jpg] [mb09095f4.jpg] |
| |||||||||
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}